Each year, an estimated 1.7 million people in the United States (US) sustain a brain injury. Many treatments are being studied to help these patients to recover and regain their normal lives — art therapy is one. Art therapy is a distinct discipline that incorporates creative methods of expression through visual art media. Art therapy, as a creative arts therapy profession, originated in the fields of art and psychotherapy and may vary i definition. This modality aids in the ecovery process by allowing the patient to do something they enjoy while working on various functional skills such as fine moto skills, gross motor skills, standing tolerance, endurance, communication, expression of feelings, relaxation, socialization, memory, and problem-solving skills. In the inpatient setting, art therapy can be used daily with both pediatric and adult patients. This form of treatment allows patients to be creative while simultaneously motivating them. The format for this type of therapy can be straightforward, for example, drawing and painting, or the approach can be much more creative. Take for example a pediatric patient with traumatic brain injury who was very interested in coloring and painting. To help with her walking and coordination, her therapist painted her feet and had her walk throughout the facility. This allowed the patient and her family to see the progress she made through the footprints she created. She was allowed to express herself daily by choosing the colors for her footprints and was motivated to continue walking more each day.

Art therapy is also being explored as a form of complementary and integrative care for military veterans affected by trauma and injuries in the line of duty includin traumatic brain injury (TBI) and post-traumatic stress disorder (PTSD). The self-soothing qualities of making art can most certainly aid in TBI recovery. Art therapy offers many psychologica and cognitive benefits for patients after a TBI and als helps improve mood, problem-solving skills, attention, and coordination. Most importantly, making art helps patients find a healthy outlet for their emotions, and ebuild their sense of self, something few other therapies can offer after traumatic brain injury.
According to John Hopkins Medicine, Body Dysmorphic Disorder (BDD) is a mental illness that causes a person to be obsessively focused on a perceived flaw in their appearance. A person with BDD may be so preoccupied with the appearance of their body that they cannot lead a normal life and may be overcome with feelings of self-hate and dissatisfaction. They may spend an excessive amount of time each day worrying about how they look, so much so that they neglect their daily responsibilities. Suicidal thoughts may also be a symptom. Some behaviors that may accompany this disorder include a person constantly checking themselves in the mirror, avoiding social activities have shown that individuals with BDD have deficiencies in this area. In one study of verbal and nonverbal memory — including visual organization strategies — subjects were asked to copy and recall a complicated figu e drawing.
The BDD group recalled more specific parts of the drawin instead of the overall structure, which may reflect poo organizational strategies marked by an imbalance in local (detail) and global information processing. Another study using the same test found impaired copying and recall in individuals with BDD. There was also evidence of impaired visual working memory as well as auditory, verbal and logical memory.
“THERE IS NO QUESTION THAT PHYSICAL DAMAGE TO THE BRAIN CAN CAUSE
COGNITIVE, EMOTIONAL, AND BEHAVIORAL ISSUES. RESEARCH HAS SHOWN THAT
THE SPECIFIC AREA OF THE BRAIN AFFECTED BY TBI TRANSLATES DIRECTLY TO THE
POTENTIAL SIDE EFFECTS A PATIENT MAY EXPERIENCE.”
- Dr. Rod Amiri, MD, Neuropsychiatrist
New research has started to identify abnormal areas and connections in the brain in hopes of developing biomarkers or brain correlates that can help identify those at risk for developing BDD. Medical research is beginning to make connections between the disorder and frontal lobe brain damage. Trauma or injury to the frontal lobe of the brain can cause a wide range of problems and changes to your personality due to the frontal lobe’s role in shaping social behavior and personal characteristics. It controls things such as personality, decision making, motivation and voluntary movements. The frontal lobe is also responsible for memory, and studies. Individuals with BDD also tend to do poorly in tasks related to decision-making, specifically those involving planning, inhibition or organization, pointing again to the frontal lobe. One study found that compared to healthy controls, those with BDD made more errors on a search task, demonstrating deficits in working memor . They also were slower on a task measuring planning ability and exhibited higher risk-taking behavior in a decision-making experiment. Based on these studies, the connection between frontal lobe abnormality and BDD is clear. However, because of the complexity of the disorder, future research is necessary to understand the exact combiniation of factors that lead to BDD.
War ravages lives across borders and cultures and within military ranks. The physical casualties [of war] are front and center, but the less talked about and equally debilitating occurrences of traumatic brain injury (TBI) are the silent wounds effecting millions globally — wounds which often goes untreated. In a conflict setting, TBI is commonly caused by blasts and leaves service members and civilians alike to grapple with life-altering cognitive difficulties, sometimes without adequate medical care to support recovery. Though the problem is more prevalent than the help, there are many agencies and organizations dedicated to assisting these victims of war.
The Office of the UN High Commissioner for Human Rights (OHCHR), the UN Assistance Mission (UNAMA), the United Nations Children’s Fund (UNICEF), and others, are dedicated to shedding light on the problem and providing solutions. SERVICE MEMBERS AND TBI According to the Joint Theater Trauma Registry, compiled by the U.S. Army Institute of Surgical Research, 22 percent of soldiers wounded in the U.S. war in Afghanistan had injuries to the head, face or neck. This percentage can serve as a rough estimate of the fraction who have TBI, according to Deborah L. Warden, a neurologist and psychiatrist at Walter Reed Army Medical Center who is the national director of the Defense and Veterans Brain Injury Center (DVBIC). Warden said the true proportion is probably higher, since some cases of closed brain injury are not diagnosed promptly.
In the Vietnam War, by contrast, 12 to 14 percent of all combat casualties had a brain injury, and an additional 2 to 4 percent had a brain injury plus a lethal wound to the chest or abdomen, according to Ronald Bellamy, former editor of the Textbooks of Military Medicine, published by the Office of the Surgeon General of the U.S. Army. Bellamy said that because mortality from brain injuries among U.S. combatants in Vietnam was 75 percent or greater, soldiers with brain injuries made up only a small fraction of the casualties treated in hospitals. Kevlar body armor and helmets are one reason for the high proportion of TBIs among soldiers wounded in more current conflicts. They work by shielding the wearer from bullets and shrapnel and have improved overall survival rates.
Kevlarhelmets have reduced the frequency of penetrating head injuries. However, the helmets cannot completely protect the face, head and neck — nor do they prevent the kind of closed brain injuries often produced by blasts. Most brain injuries in war zones are caused by improvised explosive devices (IEDs), and closed brain injuries outnumber penetrating ones among patients seen at Walter Reed, where thousands of patients with TBI are treated. All admitted patients who have been exposed to a blast are routinely evaluated for brain injury — 59 percent of them have been given a diagnosis of TBI, according to Warden.
Of these injuries, 56 percent are considered moderate or severe, and 44 percent are mild. A blast creates a sudden increase in air pressure by heating and accelerating air molecules and, immediately thereafter, a sudden decrease in pressure that produces intense wind. These rapid pressure shifts can injure the brain directly, producing concussion or contusion. Air emboli — a blockage of blood supply caused by air bubbles — can also travel to the brain, causing the death of brain tissue. When service members have serious brain injuries, they receive immediate care on the battlefield and are then transported to military combat support hospitals, where they undergo brain imaging and are treated by neurosurgeons.
Treatment may include the removal of foreign bodies, control of bleeding or craniectomy — which relieves pressure from swelling. Soldiers with TBI often have symptoms affecting several areas of brain function. Headaches, sleep disturbances and sensitivity to light and noise are common. Cognitive changes, diagnosed on mental-status examination or through neuropsychological testing, may include disturbances in attention, memory or language, as well as delayed reaction time during problem solving. Often, the most troubling symptoms are behavioral ones — mood changes, depression, anxiety, impulsiveness, emotional outbursts or inappropriate laughter.

Some symptoms of TBI overlap with those of post-traumatic stress disorder, and many effected in the military sector have both conditions. The good news is service men and women are young and healthy, and as such are in a good position to recover. CIVILIANS INJURED IN CONFLICTS The U.S. wars in Iraq, Afghanistan, Yemen, Syria and Pakistan, military operations in Somalia as well as the more recent conflict in Ukraine have taken a tremendous human toll on those countries. Hundreds of thousands of civilians have been injured as a result of these conflicts and many of these injuries have resulted in TBI. For example, according to the Watson Institute for International and Public Affairs, blast-induced TBI has been referred to as the signature injury of the conflicts in Iraq and Afghanistan. People living in these war zones have been attacked in their homes, in markets and on roadways. They have been subjected to bombs, bullets, fire and IEDs.
Civilians are victimized at checkpoints, as they are run off the road by military vehicles, when they step on mines or cluster bombs, as they collect wood or tend to their fields and when they are kidnapped and executed for purposes of revenge or intimidation. A new book, published by world-renowned UCSF neuroradiologist Dr. Alisa Gean, tackles the complexity of TBI, how it is sustained and how it affects both civilians and combatants alike. The text includes information and research gathered from nearly three decades of studying civilian TBI, as well as five intensive years of studying TBI sustained from combat, terrorism and natural disasters. “Aproximately 85% of injured World War II soldiers suffered from gunshot wounds.
Today’s enemy is using a new weapon to kill, defeat and demoralize — the improvised explosive device.” says Dr. Gean. The U.S. war in Afghanistan lasted for 22 years and resulted in an enormous footprint of civilian casualties. In their Afghanistan Protection of Civilians in Armed Conflict Annual Report, the Office of the UN High Commissioner for Human Rights (OHCHR) and the UN Assistance Mission (UNAMA) documented some 8,820 civilian casualties (3,035 deaths and 5,785 injuries) in 2020. These civilians paid a terrible price for the failure of peace negotiations and the country remains amongst the “deadliest places in the world to be a civilian”, according to Michelle Bachelet, UN High Commissioner for Human Rights. “I am particularly appalled by the high numbers of human rights defenders, journalists and media workers killed since peace negotiations began”, she says.
According to the report, the overall drop in civilian casualties in 2020 was due to fewer casualties from suicide attacks by anti-government elements in populated areas, as well as a drop in casualties attributed to international military forces. There was, however, a “worrying rise” in targeted killings by such elements — up about 45 per cent since 2019. The use of IEDs by the Taliban, air strikes by the Afghan Air
Force and ground engagements also resulted in increased casualties, according to the report. Anti-government elements bore responsibility for about 62 percent of civilian casualties, while pro-government forces were responsible for about 25 pe cent of the casualties. About 13 percent of casualties were attributed to crossfire and other incidents. The report went on to note that the years-long conflict in Afghanistan “continues to wreak a shocking and detrimental toll” on women and children, who accounted for 43 percent of all civilian casualties — 30 percent children and 13 percent women. “This report shows the acute and lasting needs of victims of the armed conflict and demonstrates how much remains to be done to meet those needs in a meaningful way”, High Commissioner Bachelet said. “The violence that has brought so much pain and suffering to the Afghan population for decades must stop and steps towards reaching a lasting peace must continue.”

June 3rd marked the 100th day of the war in Ukraine — a war that has shattered the lives of millions of children. Only days before, on June 1st, the International Day for Protection of Children [in Ukraine and across the region] was marked. “June 1 is the International Day for Protection of Children,” said UNICEF Executive Director Catherine Russell. “Instead of celebrating the occasion, we are solemnly approaching the 100th day of the war. Without an urgent ceasefire and negotiated peace, children will continue to suffer — and fallout from the war will continue to impact vulnerable children around the world.” The scale and speed of the emergency in Ukraine have not been seen since World War II, the United Nations said in a statement, which estimated that 5.2 million children in the region need humanitarian assistance; three million inside the country and more than 2.2 million in refugee-hosting countries. As intense artillery exchanges continue between Russian and Ukrainian forces in eastern Donetsk region and amid reports that Russian troops are continuing their campaign, UNICEF said that almost two in three children in Ukraine have been displaced by fighting. “Civilian infrastructure on which children depend continues to be damaged or destroyed,” the agency explained. “This so far includes at least 256 health facilities and one in six UNICEF-supported ‘Safe Schools’ in the country’s east. Hundreds of other schools across the country have also been damaged.
Conditions for children in eastern and southern Ukraine where fighting had been quite intense are increasingly desperate.” In addition to the trauma of fleeing their homes, UNICEF states that children fleeing violence faced a significant risk of family separation, abuse, sexual exploitation and trafficking. The UN agency also reiterated its call for “full humanitarian access” so that teams can “safely and quickly reach children in need wherever they may be”. Inside Ukraine, UNICEF and partners have already distributed life-saving health and medical supplies for nearly 2.1 million people in war-affected areas. Equally important, critical safe water access has also been secured for more than 2.1 million people living in areas where networks have been damaged or destroyed.
The long-lasting mental health toll of the war on children has also contributed to an acute child protection crisis, made worse by the fact that many displaced families are out of work and unable to meet their children’s basic needs. “These children urgently need safety, stability, child protection services and psychosocial support — especially those who are unaccompanied or have been separated from their families. More than anything, they need peace,” UNICEF insisted. Over 610,000 children and caregivers have also received mental health and psychosocial support, while nearly 290,000 children have been given learning supplies. In addition, almost 300,000 vulnerable families have registered for a humanitarian cash assistance program run by UNICEF and the Ukrainian Ministry of Social Policy. In countries hosting Ukrainian refugees, the UN agency continues to look out for the most vulnerable of children by providing anti-trafficking training for border guards and encouraging local authorities to integrate refugee children into schools.
Providing vaccines and medical supplies for displaced Ukrainians is a key component of UNICEF’s response, and so too is establishing play and learning hubs to provide young children with a much-needed sense of normalcy and respite. In total, 25 UNICEF-UNHCR “Blue Dots” — one-stop safe havens that provide support and services for families on the move, have been established along major transit routes in Moldova, Romania, Poland, Italy, Bulgaria and Slovakia, the agency said.
In Moldova, more than 52,000 refugees, mostly in female-headed households, have been reached through a UNICEF-UNHCR multi-purpose cash assistance program. Highlighting the devastating and lasting consequences of the war on millions of the country’s youngest citizens, UN Children’s Fund UNICEF maintains that most of the victims were from “attacks using explosive weapons in populated areas”, a claim 1.6 BILLION CHILDREN ARE LIVING IN A CONFLICT AFFECTED COUNTRY supported by the UN human rights office, OHCHR. With the use of explosive weapons, it is inevitable that many of these children will be effected by TBI. According to the Save the Children Blast Injury Report, the use of explosive weapons, traditionally meant for the open battlefield, in densely populated towns and cities continues to cause devastation to children.
Time after time, these weapons result in death, life-changing injuries and the destruction of vital facilities, such as schools and hospitals. From Syria, to Yemen, to Afghanistan, the families of the injured are left to manage TBI among other devastating injuries with health systems often at the point of collapse. And children are particularly vulnerable to blasts with their bodies being lighter, and thus easily thrown farther than an adult’s body. There are good reasons why the killing and maiming of children in conflict is defined as a grave violation by the United Nations.
If children survive explosive weapons, they often find themselves dealing not only with physical trauma and disability, but with the loss of family members, the destruction of their homes and the disruption of their education — and with it their future prospects. To say nothing of the acute stress already caused by growing up in a war zone. Though children can be quite resilient, they cannot be expected to recover without sustained and specialist support. Left untreated, the long-term effects of blast injuries will leave children facing a lifetime of suffering, and will ultimately create an entire generation at risk of exclusion. The Pediatric Blast Injury Partnership (PBIP), led by Imperial College London with Save the Children, is a practical response to the unique medical challenges faced by children with blast injuries. One of the PBIP’s most valuable resources to date is the Pediatric Blast Injury Field Manual, which gives medical staff in conflict settings, who often have to operate with little or no previous experience or training, the knowledge and technical guidance needed to treat children from the point of injury onwards. It also offers advice on how to provide long-term rehabilitation care and mental health support.
Smart initiatives like these will make a real difference to injured children, and medical institutions and humanitarian agencies like Save the Children will undoubtedly continue to build on this work to ensure children have the best chance of recovery. But in order to truly protect children in conflict, governments need to take an active role to advocate for children. This is why PBIP is calling on all warring parties to Stop the War on Children by taking steps to uphold international laws and norms, ensuring accountability for crimes against children and investing in the support necessary to help children recover from the physical and psychological trauma caused by conflict. PBIP found that 80% of pediatric blast patients experienced penetrating injuries to the head. By comparison, just 31% of adult blast patients experienced the same injury. Within this, younger children are more affected. Children under seven are almost twice as likely to present with head injuries as older children. In one study, 90% of children who died from blast injuries had skull fractures.
When children survive a blast, they are almost always left with life-limiting brain injury. Take 12-year-old Mahmoud who lives in Gaza. In 2014 when he was playing in the street, he was hit by an explosive weapon. “I heard an explosion and I felt something go into my eye. I touched my eye and felt blood pouring out. I ran for help and was taken to the hospital. I woke up missing one of my eyes.” Mahmoud’s family says byond his physical injuries, he was not himself after the accident. Mahmoud ikely suffered an undiagnosed TBI. Helle Thorning-Schmidt, CEO of Save the Children International and former Prime Minister of Denmark is uncompromising in her assessment: “International law makes clear that everyone has a responsibility to make sure children are protected in war. Yet explosive weapons continue to kill, maim and terrorize thousands of children every year. Every warring party — from armed groups to governments — must do more to protect children and abide by this important moral principle.”
The World Health Organization estimates that traumatic brain injury (TBI) is and will remain the most important cause of neurodisability in the coming years. The search for neuroprotective therapies for severe TBI has been extensive but unfruitful over the last few decades, testified by mo e than 30 failed clinical trials, and we still have no specific neu oprotective therapy, that is, effective in clinica TBI. The burden of mortality and residual disability calls for new approaches to promote recovery of function of TBI patients in the acute and chronic phase.
Classically described as a sudden event with short-term consequences, TBI induces dynamic pathological cascades that may persist for months or years after injury with a major impact on outcome. Among dynamic mechanisms, the neuroinflammatory esponse and the accumulation of aberrant proteins may have a critical role in establishing a neuropathological link between acute mechanical injury and late neurodegeneration. The close association between post-TBI neurological changes, persistent neuroinflammation, and lat neuropathology highlights the fact that the window of opportunity for therapeutic intervention may be much wider than previously thought and that long-term treatment encompassing the acute and chronic phase should be tested to effectively interfe e with this complex condition.
An emerging technology, virtual reality (VR), represents a new tool for this purpose and might provide TBI care teams with new neuro-restorative strategies readily available at the bedside. Since the late 1980s, this term has been used to describe a 3D synthetic environment created by computer graphics, where the user has the feeling of being inside. VR can be described as “an advanced form of human-computer interface that allows the user to interact with and become immersed in a computer-generated environment in a naturalistic fashion”. For its flexibilit , sense of presence (i.e., the feeling of “being there”) and emotional engagement, VR has been tested in motor and cognitive rehabilitation, with good results. In stroke patients, the number of VR programs is rapidly increasing with compelling data showing an improvement in recovery of motor function and daily living activities. VR has been successfully used both as assessment instrument and as therapeutic intervention. As assessment tool, VR has been used to detect visual-vestibular deficits in adults after concussion and mild BI. VR assessment protocols appear to be primarily implemented for mild TBI. Conversely, VR treatment protocols for cognitive rehabilitation are used transversely from mild to severe conditions, although effectiveness of thes kinds of interventions needs to be further explored.
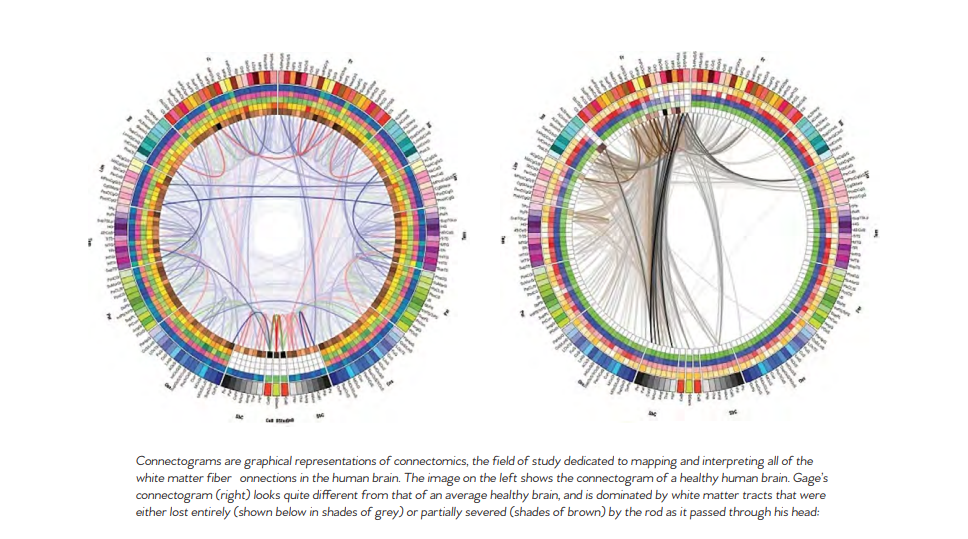
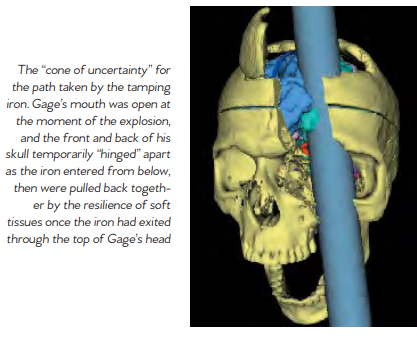
Phineas P. Gage (1823–1860) was an American railroad construction foreman remembered for his improbable survival of an accident in which a large iron rod was driven completely through his head, destroying much of his brain’s left frontal lobe, and for that injury’s reported effects on his personality and behavior over the remaining 12 years of his life. Long known as the “American Crowbar Case”—once termed “the case which more than all others is calculated to excite our wonder, impair the value of prognosis, and even to subvert our physiological doctrines” —Phineas Gage influenced 19t -century discussion about the mind and brain, particularly debate on cerebral localization, and was perhaps the first case to suggest the brain’s ole in determining personality, and that damage to specific parts of the brain might induce specific mental changes I n 1848, Gage, 25, was the foreman of a crew cutting a railroad bed in Cavendish, Vermont. On September 13, as he was using a tamping iron to pack explosive powder into a hole, the powder detonated. The tamping iron—43 inches long, 1.25 inches in diameter and weighing 13.25 pounds— shot skyward, penetrated Gage’s left cheek, ripped into his brain and exited through his skull, landing several dozen feet away. Though blinded in his left eye, he might not even have lost consciousness, and he remained savvy enough to tell a doctor that day, “Here is business enough for you.”
Gage’s initial survival would have ensured him a measure of celebrity, but his name was etched into history by observations made by John Martyn Harlow, the doctor who treated him for a few months afterward. Gage’s friends found him“no longer Gage,” Harlow wrote. The balance between his “intellectual faculties and animal propensities” seemed gone. He could not stick to plans, uttered “the grossest profanity” and showed “little deference for his fellows.” The railroad-construction company that employed him, which had thought him a model foreman, refused to take him back. So Gage went to work at a stable in New Hampshire, drove coaches in Chile and eventually joined relatives in San Francisco, where he died in May 1860, at age 36, after a series of seizures. In time, Gage became the most famous patient in the annals of neuroscience, because his case was the first to suggest a link between brain trauma and personality change. In his book An Odd Kind of Fame: Stories of Phineas Gage, the University of Melbourne’s Malcolm Macmillan writes that two-thirds of introductory psychology textbooks mention Gage. Even today, his skull, the tamping iron and a mask of his face made while he was alive are the most sought-out items at the Warren Anatomical Museum on the Harvard Medical School campus. Michael Spurlock, a database administrator in Missoula, Montana, happened upon the Wilgus daguerreotype on Flickr in December 2008. As soon as he saw the object the one-eyed man held, Spurlock knew it was not a harpoon. Too short. No wooden shaft. It looked more like a tamping iron, he thought. Instantly, a name popped into his head: Phineas Gage. Spurlock knew the Gage story well enough to know that any photograph of him would be the first to come to light. He knew enough, too, to be intrigued by Gage’s appearance, if it was Gage. Over the years, accounts of his changed character had gone far beyond Harlow’s observations, Macmillan says, turning him into an ill-tempered, shiftless drunk. But the man in the Flickr photogragh seemed well-dressed and confident It was Spurlock who told the Wilguses that the man in their daguerreotype might be Gage. After Beverly finished her online research, she and Jack concluded that the man probably was. She e-mailed a scan of the photograph to the Warren museum. Eventually it reached Jack Eckert, the public-services librarian at Harvard’s Center for the History of Medicine. “Such a ‘wow’ moment,” Eckert recalls. It had to be Gage, he determined. How many mid-19th-century men with a mangled eye and scarred forehead had their portrait taken holding a metal tool? A tool with an inscription on it? The Wilguses had never noticed the inscription; after all, the daguerreotype measures only 2.75 inches by 3.25 inches. But a few days after receiving Spurlock’s tip, Jack, a retired photography professor, was focusing a camera to take a picture of his photograph. “There’s writing on that rod!” Jack said. He couldn’t read it all, but part of it seemed to say, “through the head of Mr. Phi...”
In March 2009, Jack and Beverly went to Harvard to compare their picture with Gage’s mask and the tamping iron, which had been inscribed in Gage’s lifetime: “This is the bar that was shot through the head of Mr. Phinehas P. Gage,” it reads, misspelling the name. Harvard has not officially decl ed that the daguerreotype is of Gage, but Macmillan, whom the Wilguses contacted next, is quite certain. He has also learned of another photograph, he says, kept by a descendant of Gage’s. As for Spurlock, when he got word that his hunch was apparently correct, “I threw open the hallway door and told my wife, ‘I played a part in a historical discovery!’ ” Popular reports of Gage often depict him as a hardworking, pleasant man prior to the accident. Post-accident, these reports describe him as a changed man, suggesting that the injury had transformed him into a surly, aggressive heavy drinker who was unable to hold down a job. Harlow presented the first account of the changes in Gage’s behavior following the accident. Where Gage had been described as energetic, motivated, and shrewd prior to the accident, many of his acquaintances explained that after the injury he was “no longer Gage.” Since there is little direct evidence of the exact extent of Gage’s injuries aside from Harlow’s report, it is difficult to know exact how severely his brain was damaged. Harlow’s accounts suggest that the injury did lead to a loss of social inhibition, leading Gage to behave in ways that were seen as inappropriate. Gage’s case had a tremendous influence on early neu ology. The specific changes observed in his behavior pointed t emerging theories about the localization of brain function, or the idea that certain functions are associated with specific a eas of the brain. In those years, neurology was in its infancy. Gage’s extraordinary story served as one of the first sou ces of evidence
that the frontal lobe was involved in personality. Today, scientists better understand the role that the frontal cortex has to play in important higher-order functions such as reasoning, language, and social cognition. After the accident, Gage was unable to continue his previous job. According to Harlow, Gage spent some time traveling through New England and Europe with his tamping iron to earn money, supposedly even appearing in the Barnum American Museum in New York. He also worked briefly at a livery stabl in New Hampshire and then spent seven years as a stagecoach driver in Chile. He eventually moved to San Francisco to live with his mother as his health deteriorated. After a series of epileptic seizures, Gage died on May 21, 1860, almost 12 years after his accident. Seven years later, Gage’s body was exhumed. His brother gave his skull and the tamping rod to Dr. Harlow, who subsequently donated them to the Harvard University School of Medicine. They are still exhibited in its museum today.
Foreign accent syndrome (FAS) is a speech disorder that causes a sudden change to speech so that a native speaker is perceived to speak with a “foreign” accent. FAS is most often caused by damage to the brain caused by a stroke or traumatic brain injury. Other causes have also been reported including multiple sclerosis and conversion disorder and in some cases, no clear cause has been identified Norwegian neurologist Georg Herman Monrad-Krohn reported the best-known case of FAS, in which speech was altered in terms of timing, intonation, and tongue placement causing the subject to sound foreign. In FAS, speech remains highly intelligible and does not necessarily sound disordered. FAS has been documented in cases around the world, including accent changes from Japanese to Korean, British English to French, American English to British English, and Spanish to Hungarian.
There have been only about 100 known cases of the syndrome since it was first eported in the 1940s. The most famous case was a Norwegian woman who was hit by shrapnel in World War II; she developed a German accent and was ostracized as a result. Other cases include a British woman from Devon who developed a Chinese accent following a migraine, and another British woman who had a stroke after which she acquired a French accent. FAS affects only a small a ea of speech — the pattern and intonation — and in some recorded cases appears to have been brought on by a stroke or traumatic brain injury (TBI). The primary symptom of foreign accent syndrome is speaking in an accent associated with a country where the person has never lived or in a language, they have never spoken. For example, a native English speaker who has never left the United States may begin speaking English with a
Spanish accent. Most people with foreign accent syndrome also show symptoms of a psychological or neurological condition. They might have schizophrenia or depression, a recent brain injury, or a medical condition, such as MS or dementia, that damages the brain. A person whose foreign accent changes slightly or who develops a new accent after living abroad would not be considered to have foreign accent syndrome. A person with foreign accent syndrome may seek treatment because they or someone they know noticed the change in their speech. In some cases, however, foreign accent syndrome presents secondary to another symptom. In this scenario, a person seeking emergency psychiatric care might also have an unusual accent, or a head injury survivor may develop a new speech pattern. No specific test can assess for fo eign accent syndrome. Instead, doctors work to diagnose the cause using a variety of tests, including blood tests to test for infections and some illnesses, brain scans, such as MRI scans, to look for lesions or damage in the brain, a lumbar puncture, to test for infections in the spinal flui and to check for signs of certain central nervous system conditions, a complete medical history, to determine when the symptoms
appeared and what may have caused them, and psychiatric screenings, such as assessments for depression and schizophrenia. If a doctor cannot find a physiological cause, they will usuall diagnose a person with psychogenic foreign accent syndrome and work to identify a possible psychological cause. Foreign accent syndrome itself is not dangerous. However, it may warn of a serious medical condition, such as a tumor or lesion in the brain, dementia, or MS. In these cases, treatment will focus on addressing the cause of the foreign accent syndrome. A doctor might prescribe medication for conditions such as MS or surgery for certain brain growths. When there is a psychiatric cause, a doctor may recommend therapy, medication, or both. Many causes of foreign accent syndrome are not curable, though medication can help manage symptoms. In most cases, a doctor will recommend speech therapy to help a person regain their normal habits. When the cause of foreign accent syndrome is unclear — such as in the case of the woman who developed it following dental surgery — speech therapy may be the only treatment option
Traumatic Brain Injury (TBI) disrupts the normal functioning of the brain due to a strike or jolt to the head. This can cause vision problems, such as blurred or double vision, and difficulty wi eye movements, focus, and tracking. This can result in headaches, dizziness and nausea— especially when someone who has suffe ed a TBI needs to retain focus on a fixed poin or task. Over 10 million TBIs occur annually around the world and around 57 million people have been hospitalized for a TBI at some point in their lives. Studies show that over 90% of Traumatic Brain Injury patients suffer some form of visua dysfunction, yet vision problems tend to be overlooked during the initial treatment of a brain injury. At times, vision problems don’t manifest until some time has passed— so make sure to pay close attention to any vision changes you may experience following a concussion or head trauma. If you notice any alterations in your vision, contact our optometrists right away. The eye doctor will determine the causes of the vision change and will provide the appropriate vision therapy treatment
Often the affected person with a TBI is not aware of their specific vision dysfunction but might complain of one or more of the signs below: Traumatic Brain Injuries tend to interrupt the communication between the eyes and the brain, which can cause a range of visual dysfunctions. The signs often include: - Blurred vision - Eyestrain - Sensitivity to light - Reading difficulti - Attention and concentration difficulti Below is a more detailed list of the common vision problems that can result from brain injury or a medical condition, such as a stroke, tumor, aneurysm, meningitis, cerebral palsy, and other neurological insults. Visual Acuity – Blurry vision, either all the time or can shift in and out of focus. Eye focusing – Inability to quickly change focus from near to far objects. Eye teaming – The eyes not working in tandem, potentially causing double vision.
Eye Movements – Difficulty following a movin object or losing one’s place while reading. Motion Sensitivity – The disruption of the connection between vision integration and balance system which makes it difficult t process motion properly. This can cause vertigo or unease when traveling, scrolling a digital device, or when in busy environments such as grocery stores, social settings, or sporting events. Visual Field Loss – The partial or complete loss of peripheral vision. Visual field loss may cause one to bump into objects, be struck by approaching objects, or experience frequent falls. Visual Memory Loss – Losing the ability to recall or remember visual information stored in long or short-term visual memory. This can have a devastating impact on daily functioning as the individual no longer recalls numbers, words, pictures, or any data viewed in the past. Reading comprehension decreases, and the ability to recognize locations and faces declines. One may not remember where a specific object—such as a car key—was put or how to give directions. Headaches or Eye Pain – Following head trauma, the individual may experience a range of headaches or even a stabbing pain around the eye — at times accompanied by redness, burning, or itching of the eyes Sensitivity to Light – In the aftermath of a brain injury, one can develop sensitivity to light and be unable to tolerate glare. Also known as photophobia, sensitivity to light can be exacerbated by particular light sources, such as bright sunlight and fluo escent lighting. LCD screens, used for computers or smartphone devices, can be particularly intolerable after a concussion. People of all ages who develop visual dysfunction due to a neurological trauma or injury can benefit f om a vision assessment by a Neuro-Optometric Rehabilitation Optometrist (neuro-optometrist). These eye care professionals are highly trained in the diagnosis, treatment and rehabilitation of neurological conditions that affec the visual system, as well as perceptual and motor disorders. Research studies show that patients having undergone a vision rehabilitation program can vastly improve their quality of life. An interdisciplinary rehabilitation team is essential for patients with concussions, strokes or other neurological deficits. In addition t optometrists, team members may include nurses, physical therapists, occupational therapists, speechlanguage pathologists, physical medicine doctors, neurologists, neuropsychologists, audiologists, and ophthalmologists, among others.
Mild or moderate COVID-19 lasts about two weeks for most people. But in some, the long-term effects of COVID-19 can cause lingering health problems and wreak havoc for months. Tae Chung, M.D., a specialist in neurology and physical medicine and rehabilitation; Megan Hosey, Ph.D., an expert in rehabilitation psychology; Arun Venkatesan, M.D., Ph.D., a specialist in neurology; Amanda Morrow, M.D., an expert in pediatric rehabilitation medicine; and Ann M. Parker, M.D., Ph.D., who specializes in lung disease and critical care, discuss long-term COVID-19, what symptoms are most common and what those affected by them can expect Mild or moderate COVID-19 lasts about two weeks for most people. But others experience lingering health problems even after the fever and cough go away and they are no longer testing positive for the illness.
Parker notes that the World Health Organization has developed a definition for post-COVID-19 condition (the WHO’s term for long COVID) as coronavirus symptoms that persist or return three months after a person becomes ill from infection with SARS CoV-2, the coronavirus that causes COVID-19. Those symptoms can include fatigue, shortness of breath and cognitive problems. The symptoms can come and go, but have an impact on the person’s everyday functioning, and cannot be explained by another health problem. WHAT CAUSES POST-COVID SYNDROME? While it’s clear that people with certain risk factors (including high blood pressure, smoking, diabetes, obesity and other conditions) are more likely to have a serious bout of COVID-19, there isn’t a clear link between these risk factors and long-term problems. In fact, long COVID can happen in people who have mild symptoms, although patients with more severe initial illness seem to be more likely to have long-term impairments.
More studies will shed light on why these stubborn health problems persist in some people. SARS-CoV-2 can attack the body in a range of ways, causing damage to the lungs, heart, nervous system, kidneys, liver and other organs. Mental health problems can arise from grief and loss, unresolved pain or fatigue, or from post-traumatic stress disorder (PTSD) after treatment in the intensive care unit (ICU).
Doctors are seeing a spectrum of symptoms after acute COVID-19, some of which would be expected after other critical illnesses. Some are minor, but other people may need continuing care and even readmission to the hospital. Similar, lingering problems can affect patients with other serious illnesses. But it is notable that post-COVID-19 syndrome is not just afflicting people who were very sick with the coronavirus: Some patients who were never severely ill with COVID-19 are experiencing long-term symptoms.
DO COVID VACCINES PREVENT LONG COVID?
Getting vaccinated for COVID-19 lowers the risks of COVID infection. While breakthrough infections are possible, being fully vaccinated and boosted is effective in reducing the risk of hospitalization and death due to COVID. Research is ongoing about how long COVID affects people who had breakthrough COVID, but it is likely that being vaccinated reduces the risk.
POST-COVID SYNDROME CONDITIONS
The senses of smell and taste are related, and because the coronavirus can affect cells in the nose, having COVID-19 can result in lost or distorted senses of smell (anosmia) or taste. Before and after people become ill with COVID-19, they might lose their sense of smell or taste entirely, or find that familiar things smell or taste bad, strange or different. For about a quarter of people with COVID-19 who have one or both of these symptoms, the problem resolves in a couple of weeks. But for most, these symptoms persist. Though not life-threatening, prolonged distortion of these senses can be devastating and can lead to lack of appetite, anxiety and depression. Some studies suggest that there’s a 60% to 80% chance that these people will see improvement in their sense of smell within a year. Neurologist Arun Venkatesan, M.D., Ph.D., says, “Some individuals develop medium to long-term symptoms following COVID infection, including brain fog, fatigue, headaches and dizziness. The cause of these symptoms is unclear but is an active area of investigation
Can COVID-19 increase a person’s risk for anxiety, depression and cognitive issues? A study of COVID-19’s impact on mental and emotional well-being conducted by Johns Hopkins experts in psychiatry, cognition (thinking, reasoning and remembering) and mental health found that these problems were common among a diverse sample of COVID-19 survivors. Cognitive impairment after acute coronavirus infection can have a severe impact on a person’s life. Long-haul COVID patients may experience changes in the way they think, concentrate, speak and remember, and these symptoms can affect their ability to work or even maintain activities of daily living. After recovering from the coronavirus, some people are left with lingering anxiety, depression and other post-COVID mental health issues.
Physical changes such as pain and weakness can be complicated by long periods of isolation, stress from job loss and financial difficulties, and grief from the deaths of loved ones and the loss of good health. The relationship between COVID-19 and diabetes, especially type 2 diabetes, is complex. Type 2 diabetes is a risk factor for serious cases of COVID-19, and some survivors of the illness seem to be developing type 2 diabetes signs after they recover from COVID-19. It’s not yet known whether children who have had COVID-19 are more or less likely than adults to experience continuing symptoms. But long-term COVID-19 in children is a possibility, showing up as fatigue, headaches, difficulty with school work, mood concerns, shortness of breath and other long-hauler symptoms.
SEVERE POST-COVID COSTOCHONDRITIS
Although children comprise the fewest cases of COVID-19 infection, symptoms and complications among the various age groups affected, new long-term consequences a e being reported including severe costochondritis. Post-COVID costochondritis (PCC) is an inflammation of the cartilage that connects a rib to the breastbone. The syndrome causes pain and tenderness on the breastbone, pain in more than one rib, or pain that gets worse with deep breaths or coughing. Patients will experience sharp or aching pain which can start suddenly or develop slowly and spread across the chest. Because of the location of the pain, the symptoms are sometimes misinterpreted as a heart attack. Costochondritis usually goes away on its own, although it might last for several weeks or longer. Treatment focuses on pain relief with traditional treatments including injections to relieve pain and medications — though PCC, in many cases, is unresonsive to these treatments. Physical therapy in the form of gentle stretching exercises for the chest muscles might be helpful. Medications used to treat PCC may include nonsteroidal anti-inflammatory d ugs. Some of these drugs, such as ibuprofen
(Advil, Motrin IB) or naproxen sodium (Aleve), can be purchased over the counter. Stronger versions are available by prescription. Side effects of these medicines can include damage to th stomach lining and kidneys. Narcotics may also be used if pain is severe, however, are avoided when possible because they can be habit-forming. Antidepressants such as amitriptyline are often used to control chronic pain — especially if the pain interferes with sleep and anti-seizure medication such as gabapentin (Gralise, Neurontin) has also proved successful in controlling chronic pain caused by PCC. In a study conducted at the School of Medicine, Texas Tech University Health Sciences Center in Lubbock, Texas, researchers found that PCC in some cases may respond to treatment with colchicine, an anti-inflammator . Another option is a procedure called transcutaneous electrical nerve stimulation (TENS), in which a device sends a weak electrical current via adhesive patches on the skin near the area of pain. The current is thought to possibly interrupt pain signals, preventing them from reaching the brain. If conservative measures are not successful, the injection of numbing medication and a corticosteroid directly into the painful joint is also an option.


CARDIOVASCULAR CONDITIONS
A study published in Nature Medicine by researchers at the Veterans Affairs ( A) St Louis Health Care System, found that in the year after recovering from the illness’s acute phase, patients had increased risks of an array of cardiovascular problems, including abnormal heart rhythms, heart muscle inflammation, blood clots, st okes, myocardial infarction, and heart failure. What’s more, the heightened risks were evident even among those who weren’t hospitalized with acute COVID-19. Patients with more severe disease—determined by whether they recuperated at home, were hospitalized, or were admitted to the intensive care unit—had higher risks. But the risks were evident even among those who were not hospitalized with COVID-19. Other subgroup analysis found increased risks regardless of age, race, sex, obesity, smoking, hypertension, diabetes, chronic kidney disease, hyperlipidemia and preexisting cardiovascular disease.
RESPIRATORY ISSUES
Severe cases of COVID-19 can produce scarring and other permanent problems in the lungs. This is likely due to a combination of the body’s exaggerated immune system reaction to the virus, and the lung inflammation it triggers. Even mil infections can result in persistent respirtory distress — causing shortness of breath after even light exertion. Lung recovery after COVID-19 is possible, but takes time. Experts say it can take months for a person’s lung function to return to pre-COVID-19 levels. Breathing exercises and respiratory therapy can help. Researchers from the University of Iowa recently conducted a study to understand the long-term effects of COVID-19 on lun function. The study enrolled 100 adults with a confirmed SARS CoV-2 infection who remained symptomatic for more than 30 days following the diagnosis, with a control group of 106 healthy participants. The results provided evidence of airway damage many months after the initial SARS CoV-2 infection.
CHRONIC FATIGUE
A team of researchers, including two from Johns Hopkins Medicine, have published a review article highlighting similarities between certain lingering symptoms following COVID-19 illness — a condition called “long COVID” — and myalgic encephalomyelitis/chronic fatigue syndrome (ME/ CFS), a debilitating, complex disorder previously known as chronic fatigue syndrome. The researchers say the symptoms shared by the two conditions may involve a biological response that goes haywire when the body encounters certain infections or other environmental hazards. “The body’s response to infection and injury is complex and covers all body systems,” says the study’s lead author Bindu Paul, Ph.D., assistant professor of pharmacology and molecular sciences at the Johns Hopkins University School of Medicine. “When that response is in disarray — even just one aspect of it — it can cause feelings of being tired, brain fog, pain and other symptoms.”
LOSS OF TASTE AND SMELL
The senses of smell and taste are related, and because the coronavirus can affect cells in the nose, having COVID-19 can result in lost or distorted senses of smell (anosmia) or taste. Before and after people become ill with COVID-19, they might lose their sense of smell or taste entirely, or find that familiar things smell or taste bad, strange or diffe ent. For about a quarter of people with COVID-19 who have one or both of these symptoms, the problem resolves in a couple of weeks. But for most, these symptoms persist. Though not life-threatening, prolonged distortion of these senses can be devastating and can lead to lack of appetite, anxiety and depression. Some studies suggest that there’s a 60% to 80% chance that these people will see improvement in their sense of smell within a year
MUSCULOSKELETAL CONDITIONS
Recent studies have suggested that musculoskeletal symptoms, including joint and muscle pain, are present in many COVID-19 patients after the acute phase of infection, persisting for weeks or even months after the initial infection. Comprising 40% of the human body weight, the skeletal muscle is an important organized tissue composed by numerous bundles of myofibers. It has a crucial mechanical role, generating force and power through the conversion of chemical to mechanical energy, which yields movement, facilitating our daily activities. Furthermore, skeletal muscle can store energetic substrates (carbohydrates and amino acids) for the basal metabolism and it can contribute to heat production, stabilizing the body’s temperature. Considering the multiple functions of the musculoskeletal system and the fact that COVID-19 is a multi-organic disease, it isn’t surprising that musculoskeletal issues may arrise from infection.
SLEEP DISORDERS
“Sleep disorders are one of the most common symptoms for patients who’ve had COVID-19,” says sleep medicine specialist Cinthya Pena Orbea, MD. “They report insomnia, fatigue, brain fog and sometimes we even see circadian rhythm disorders.” Coined “coronasomnia,” COVID-19- induced insomnia is often attributed to pandemic-related stress, anxiety, depression and other mental health conditions. According to Dr. Orbea, many people have a delayed sleep cycle, causing them to fall asleep much later in the evening or earlier in the morning. This delayed cycle extends into the following day, causing people to feel groggy, have chronic fatigue or wake up later than they prefer. “Sleep is extremely important for the overall function of our bodies, including our metabolic systems and our immune systems,” explains Dr. Orbea. “Since sleep is important for concentration and memory function, it will enhance how patients recover from the disease and impact their quality of life.” During illness, the immune system’s response to an infection can have a profound effect on sleep. Likewise, getting adequate, good quality sleep is crucial for your immune system to work optimally. In long COVID, if the immune system is still not functioning normally, the body will be constantly trying its hardest to reduce the inflammation. This could explain why so many people with long COVID report fatigue and sleep difficulties as major symptoms. It’ also thought that inflammation can come and go during long COVID, which would mean that the body is constantly having to work to keep everything in balance. When the body is having to deal with chronic inflammation, sleep can be reduced and sleep quality can be compromised.
PERIPHERAL NEUROPATHY
Some patients with long COVID may have long-lasting nerve damage resulting in weakness, numbness and pain, usually in the hands and feet. This condition , known as peripheral neuropathy, appears to be caused by immunity problems triggered by infection according to a new study published in the journal Neurology: Neuroimmunology & Neuroinflammation. “This is one of the early papers looking into causes of long COVID, which will steadily increase in importance as acute COVID wanes,” said Anne Louise Oaklander, MD, the lead study author and a neurologist at Massachusetts General Hospital. “Our findings suggest that some long COVID patients had damage to their peripheral nerve fibers and that damage to the small-fiber type of nerve cell may be prominent.” The study found that 10 patients — or 59% — had at least one test that confirmed neuropathy. Two patients had rare neuropathies that affected muscle nerves and 10 were diagnosed with small-fiber neuropathy, which is a cause of chronic pain. Common symptoms included fatigue, weakness, changes in their senses, and pain in their hands and feet.

COGNITIVE DEFICITS
Post COVID neurological problems have been commonly reported and include cognitive or memory disturbances, headache and myalgia. Acute neurological diagnoses include encephalopathy, delirium, cerebrovascular disease, seizures, neuropathy and myopathy. Less frequently reported problems include abnormal movements, psychomotor agitation, syncope and autonomic dysfunction. Another common complaint amongst post COVID patients is brain fog, a term used to describe slow or sluggish thinking. Brain fog can occur under many different circumstances — for example, when someone is sleep-deprived or feeling unwell, or due to side effects from medicines that cause drowsiness. Brain fog can also occur following chemotherapy or a concussion. In many cases, brain fog is temporary and gets better on its own. However, we don’t really understand why brain fog happens after COVID-19, or how long these symptoms are likely to last. But we do know that this form of brain fog can affect different aspects of cognition.
Among patients hospitalized with COVID-19, 1 year after discharge, about half experienced clinically relevant moderate or worse diminished cognitive ability in verbal learning and executive function, according to study findings published in European Neuropsychopharmacology. Lingering cognitive, neurologic, psychiatric, and physical symptoms after COVID are estimated to affect as many as 40 of all patients who contracted COVID-19 and as much as 85% of those who have been hospitalized with COVID-19. Cognitive COVID (which is long-term) is characterized by brain fog, and memory and concentration struggles, and is recognizable in about 30% of patients previously hospitalized with the virus. COVID infection frequently leads to brain damage — particularly in those over 70. While sometimes the brain damage is obvious and leads to major cognitive impairment, more frequently the damage is mild, leading to difficulties with sustained atte ion. Although many people who have recovered from COVID can resume their daily lives without difficulty — even if they ha some deficits in attention — the e are a number of people who may experience difficulty for an extended period
Diagnosing TBI can be complicated. Currently, doctors use a variety of methods to determine if a patient has a TBI. A medical exam is the first step to diagnose a potential brain injury which includes a neurological exam. This exam evaluates thinking motor function, sensory function, coordination, eye movement, and reflexes. Although it is well acknowledged within the medical community that they can not detect TBIs, CT and MRI scans are typically the next step because they can rule out a more serious brain injury. Although these protocols aid health care providers who are trained in the intricacies of diagnosing TBIs, none on their own can provide a definitive diagnosis. However, there is promising research showing that more advanced imaging may take center stage in the diagnosis of both TBI and mTBI (mild traumatic brain injury).
This next-level imaging falls into two categories: Nuclear Medicine in the form of single-photon emission computerized tomography (SPECT) and positron emission tomography (PET) scans and Diffusion Tensor Imaging (DTI) scans.
SPECT AND PET SCANS
SPECT is a nuclear imaging scan that integrates computed tomography (CT) and a radioactive tracer. The tracer is what allows doctors to see how blood flows to brain tissue. Before the SPECT scan, a tracer is injected into your bloodstream. The tracer is radiolabeled, meaning it emits gamma rays that can be detected by the CT scanner. The computer collects the information emitted by the gamma rays and displays it on the CT cross-sections. These cross-sections can be added back together to form a 3D image of your brain. The radioactive tracers will pass through your body and be detected by the scanner.
PET scans also use radiotracers however for additional purposes other than monitoring blood flow. PET scans also visualize and measure and physiological processes such as regional chemical composition and absorption. In both SPECT and PET scans, different tracers are used depending on the purpose of the scan. In the case of TBI screening, Fluorodeoxyglucose (FDG) is the most widely used radiotracer.
A SPECT scan differs from a PET scan in that with SPECT the tracer stays in your bloodstream rather than being absorbed by surrounding tissues, thereby limiting the images to areas where blood flows. SPECT scans are cheaper and more readily available than higher resolution PET scans, though both scans can detect minute molecular biological changes in the brain, which is not possible for MRI or CT scans.
According to Dr. Daniel Amen, a brain health expert, “Brain SPECT imaging identifies areas of the brain hurt by TBI. CT and MRI scans show if there is any damage to the anatomy or structure of your brain, but these scans cannot tell how your brain is functioning. In fact, after a TBI, CT or MRI scans will often appear normal when there is actually functional damage to the brain that can be detected with SPECT.”
DTI SCAN
DTI scans are a relatively new magnetic resonance imaging (MRI) technique that is used to evaluate microstructural changes in the brain by measuring water molecules in tissue. Its imaging capabilities are based on the ability to determine the orientation and diffusion characteristics of white matter. Recent advances in the resolution of DTI have made it possible to visualize potential changes in various neural tracts associated with brain injury. DTI is used in conjunction with conventional MRI techniques to provide 2-dimensional and 3-dimensional visualization of changes to white matter in the brain. DTI scans can provide image contrast that was previously unattainable using conventional MRI techniques.
According to Lauren J. O’Donnell, PhD of the Golby Neurosurgical Brain Mapping Laboratory, DTI is a sensitive probe of cellular structure that works by measuring the diffusion of water molecules. Unlike the diffusion in a glass of pure water, which would be the same in all directions (isotropic), the diffusion measured in tissue varies with direction (is anisotropic). The measured macroscopic diffusion anisotropy is due to microscopic tissue heterogeneity. In the white matter of the brain, diffusion anisotropy is primarily caused by cellular membranes, with some contribution from myelination and the packing of the axons. Anisotropic diffusion can indicate the underlying tissue orientation.
WHAT ADVANCED IMAGING TECHNIQUES MEAN FOR TBI PATIENTS
Being able to thrive with TBI means getting the proper diagnosis, which is the first step in getting the appropriate treatment. SPECT, PET, and DTI scans are making this possible for more patients. The amount of detail and diagnostic information made available by these scans can help doctors create very customized treatment plans for patients with TBI.
With more research being done every year to develop advanced imaging modalities, the future is definitely brighter for patients suffering from TBI.
Contribute to the TBI Times