The World Health Organization estimates that traumatic brain injury (TBI) is and will remain the most important cause of neurodisability in the coming years. The search for neuroprotective therapies for severe TBI has been extensive but unfruitful over the last few decades, testified by mo e than 30 failed clinical trials, and we still have no specific neu oprotective therapy, that is, effective in clinica TBI. The burden of mortality and residual disability calls for new approaches to promote recovery of function of TBI patients in the acute and chronic phase.
Classically described as a sudden event with short-term consequences, TBI induces dynamic pathological cascades that may persist for months or years after injury with a major impact on outcome. Among dynamic mechanisms, the neuroinflammatory esponse and the accumulation of aberrant proteins may have a critical role in establishing a neuropathological link between acute mechanical injury and late neurodegeneration. The close association between post-TBI neurological changes, persistent neuroinflammation, and lat neuropathology highlights the fact that the window of opportunity for therapeutic intervention may be much wider than previously thought and that long-term treatment encompassing the acute and chronic phase should be tested to effectively interfe e with this complex condition.
An emerging technology, virtual reality (VR), represents a new tool for this purpose and might provide TBI care teams with new neuro-restorative strategies readily available at the bedside. Since the late 1980s, this term has been used to describe a 3D synthetic environment created by computer graphics, where the user has the feeling of being inside. VR can be described as “an advanced form of human-computer interface that allows the user to interact with and become immersed in a computer-generated environment in a naturalistic fashion”. For its flexibilit , sense of presence (i.e., the feeling of “being there”) and emotional engagement, VR has been tested in motor and cognitive rehabilitation, with good results. In stroke patients, the number of VR programs is rapidly increasing with compelling data showing an improvement in recovery of motor function and daily living activities. VR has been successfully used both as assessment instrument and as therapeutic intervention. As assessment tool, VR has been used to detect visual-vestibular deficits in adults after concussion and mild BI. VR assessment protocols appear to be primarily implemented for mild TBI. Conversely, VR treatment protocols for cognitive rehabilitation are used transversely from mild to severe conditions, although effectiveness of thes kinds of interventions needs to be further explored.
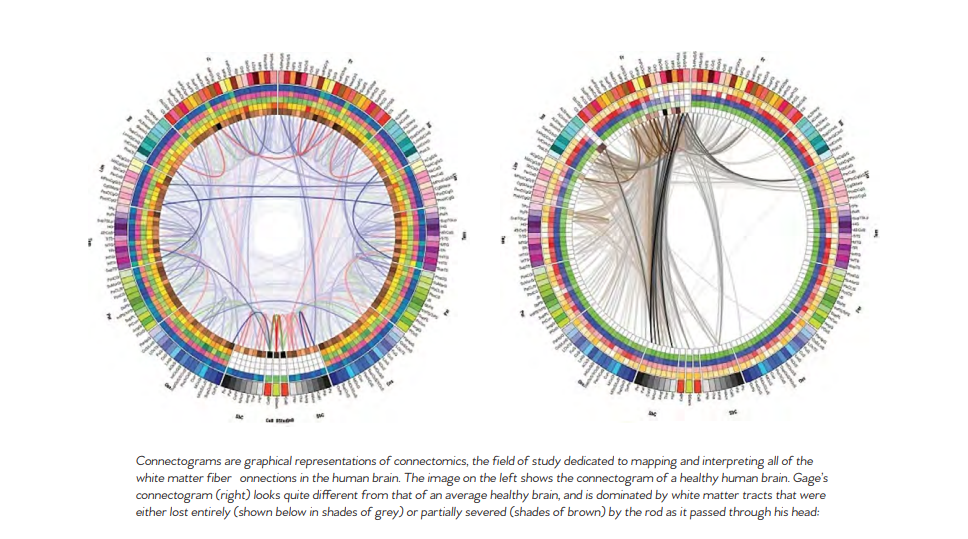
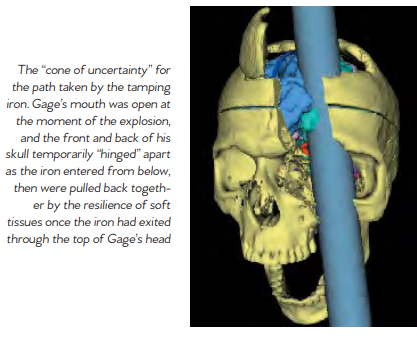
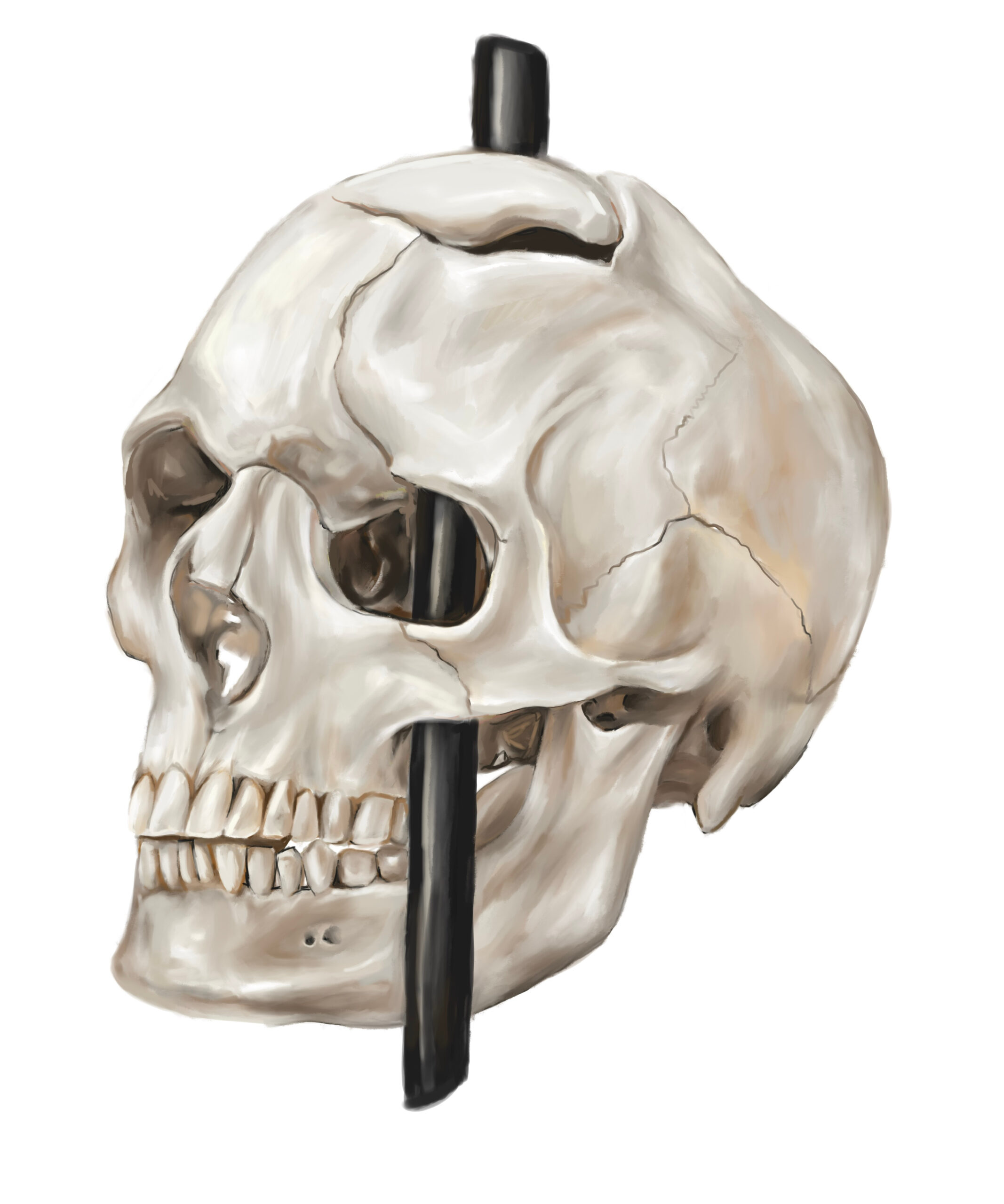
Phineas P. Gage (1823–1860) was an American railroad construction foreman remembered for his improbable survival of an accident in which a large iron rod was driven completely through his head, destroying much of his brain’s left frontal lobe, and for that injury’s reported effects on his personality and behavior over the remaining 12 years of his life. Long known as the “American Crowbar Case”—once termed “the case which more than all others is calculated to excite our wonder, impair the value of prognosis, and even to subvert our physiological doctrines” —Phineas Gage influenced 19t -century discussion about the mind and brain, particularly debate on cerebral localization, and was perhaps the first case to suggest the brain’s ole in determining personality, and that damage to specific parts of the brain might induce specific mental changes I n 1848, Gage, 25, was the foreman of a crew cutting a railroad bed in Cavendish, Vermont. On September 13, as he was using a tamping iron to pack explosive powder into a hole, the powder detonated. The tamping iron—43 inches long, 1.25 inches in diameter and weighing 13.25 pounds— shot skyward, penetrated Gage’s left cheek, ripped into his brain and exited through his skull, landing several dozen feet away. Though blinded in his left eye, he might not even have lost consciousness, and he remained savvy enough to tell a doctor that day, “Here is business enough for you.”
Gage’s initial survival would have ensured him a measure of celebrity, but his name was etched into history by observations made by John Martyn Harlow, the doctor who treated him for a few months afterward. Gage’s friends found him“no longer Gage,” Harlow wrote. The balance between his “intellectual faculties and animal propensities” seemed gone. He could not stick to plans, uttered “the grossest profanity” and showed “little deference for his fellows.” The railroad-construction company that employed him, which had thought him a model foreman, refused to take him back. So Gage went to work at a stable in New Hampshire, drove coaches in Chile and eventually joined relatives in San Francisco, where he died in May 1860, at age 36, after a series of seizures. In time, Gage became the most famous patient in the annals of neuroscience, because his case was the first to suggest a link between brain trauma and personality change. In his book An Odd Kind of Fame: Stories of Phineas Gage, the University of Melbourne’s Malcolm Macmillan writes that two-thirds of introductory psychology textbooks mention Gage. Even today, his skull, the tamping iron and a mask of his face made while he was alive are the most sought-out items at the Warren Anatomical Museum on the Harvard Medical School campus. Michael Spurlock, a database administrator in Missoula, Montana, happened upon the Wilgus daguerreotype on Flickr in December 2008. As soon as he saw the object the one-eyed man held, Spurlock knew it was not a harpoon. Too short. No wooden shaft. It looked more like a tamping iron, he thought. Instantly, a name popped into his head: Phineas Gage. Spurlock knew the Gage story well enough to know that any photograph of him would be the first to come to light. He knew enough, too, to be intrigued by Gage’s appearance, if it was Gage. Over the years, accounts of his changed character had gone far beyond Harlow’s observations, Macmillan says, turning him into an ill-tempered, shiftless drunk. But the man in the Flickr photogragh seemed well-dressed and confident It was Spurlock who told the Wilguses that the man in their daguerreotype might be Gage. After Beverly finished her online research, she and Jack concluded that the man probably was. She e-mailed a scan of the photograph to the Warren museum. Eventually it reached Jack Eckert, the public-services librarian at Harvard’s Center for the History of Medicine. “Such a ‘wow’ moment,” Eckert recalls. It had to be Gage, he determined. How many mid-19th-century men with a mangled eye and scarred forehead had their portrait taken holding a metal tool? A tool with an inscription on it? The Wilguses had never noticed the inscription; after all, the daguerreotype measures only 2.75 inches by 3.25 inches. But a few days after receiving Spurlock’s tip, Jack, a retired photography professor, was focusing a camera to take a picture of his photograph. “There’s writing on that rod!” Jack said. He couldn’t read it all, but part of it seemed to say, “through the head of Mr. Phi...”
In March 2009, Jack and Beverly went to Harvard to compare their picture with Gage’s mask and the tamping iron, which had been inscribed in Gage’s lifetime: “This is the bar that was shot through the head of Mr. Phinehas P. Gage,” it reads, misspelling the name. Harvard has not officially decl ed that the daguerreotype is of Gage, but Macmillan, whom the Wilguses contacted next, is quite certain. He has also learned of another photograph, he says, kept by a descendant of Gage’s. As for Spurlock, when he got word that his hunch was apparently correct, “I threw open the hallway door and told my wife, ‘I played a part in a historical discovery!’ ” Popular reports of Gage often depict him as a hardworking, pleasant man prior to the accident. Post-accident, these reports describe him as a changed man, suggesting that the injury had transformed him into a surly, aggressive heavy drinker who was unable to hold down a job. Harlow presented the first account of the changes in Gage’s behavior following the accident. Where Gage had been described as energetic, motivated, and shrewd prior to the accident, many of his acquaintances explained that after the injury he was “no longer Gage.” Since there is little direct evidence of the exact extent of Gage’s injuries aside from Harlow’s report, it is difficult to know exact how severely his brain was damaged. Harlow’s accounts suggest that the injury did lead to a loss of social inhibition, leading Gage to behave in ways that were seen as inappropriate. Gage’s case had a tremendous influence on early neu ology. The specific changes observed in his behavior pointed t emerging theories about the localization of brain function, or the idea that certain functions are associated with specific a eas of the brain. In those years, neurology was in its infancy. Gage’s extraordinary story served as one of the first sou ces of evidence
that the frontal lobe was involved in personality. Today, scientists better understand the role that the frontal cortex has to play in important higher-order functions such as reasoning, language, and social cognition. After the accident, Gage was unable to continue his previous job. According to Harlow, Gage spent some time traveling through New England and Europe with his tamping iron to earn money, supposedly even appearing in the Barnum American Museum in New York. He also worked briefly at a livery stabl in New Hampshire and then spent seven years as a stagecoach driver in Chile. He eventually moved to San Francisco to live with his mother as his health deteriorated. After a series of epileptic seizures, Gage died on May 21, 1860, almost 12 years after his accident. Seven years later, Gage’s body was exhumed. His brother gave his skull and the tamping rod to Dr. Harlow, who subsequently donated them to the Harvard University School of Medicine. They are still exhibited in its museum today.
Foreign accent syndrome (FAS) is a speech disorder that causes a sudden change to speech so that a native speaker is perceived to speak with a “foreign” accent. FAS is most often caused by damage to the brain caused by a stroke or traumatic brain injury. Other causes have also been reported including multiple sclerosis and conversion disorder and in some cases, no clear cause has been identified Norwegian neurologist Georg Herman Monrad-Krohn reported the best-known case of FAS, in which speech was altered in terms of timing, intonation, and tongue placement causing the subject to sound foreign. In FAS, speech remains highly intelligible and does not necessarily sound disordered. FAS has been documented in cases around the world, including accent changes from Japanese to Korean, British English to French, American English to British English, and Spanish to Hungarian.
There have been only about 100 known cases of the syndrome since it was first eported in the 1940s. The most famous case was a Norwegian woman who was hit by shrapnel in World War II; she developed a German accent and was ostracized as a result. Other cases include a British woman from Devon who developed a Chinese accent following a migraine, and another British woman who had a stroke after which she acquired a French accent. FAS affects only a small a ea of speech — the pattern and intonation — and in some recorded cases appears to have been brought on by a stroke or traumatic brain injury (TBI). The primary symptom of foreign accent syndrome is speaking in an accent associated with a country where the person has never lived or in a language, they have never spoken. For example, a native English speaker who has never left the United States may begin speaking English with a
Spanish accent. Most people with foreign accent syndrome also show symptoms of a psychological or neurological condition. They might have schizophrenia or depression, a recent brain injury, or a medical condition, such as MS or dementia, that damages the brain. A person whose foreign accent changes slightly or who develops a new accent after living abroad would not be considered to have foreign accent syndrome. A person with foreign accent syndrome may seek treatment because they or someone they know noticed the change in their speech. In some cases, however, foreign accent syndrome presents secondary to another symptom. In this scenario, a person seeking emergency psychiatric care might also have an unusual accent, or a head injury survivor may develop a new speech pattern. No specific test can assess for fo eign accent syndrome. Instead, doctors work to diagnose the cause using a variety of tests, including blood tests to test for infections and some illnesses, brain scans, such as MRI scans, to look for lesions or damage in the brain, a lumbar puncture, to test for infections in the spinal flui and to check for signs of certain central nervous system conditions, a complete medical history, to determine when the symptoms
appeared and what may have caused them, and psychiatric screenings, such as assessments for depression and schizophrenia. If a doctor cannot find a physiological cause, they will usuall diagnose a person with psychogenic foreign accent syndrome and work to identify a possible psychological cause. Foreign accent syndrome itself is not dangerous. However, it may warn of a serious medical condition, such as a tumor or lesion in the brain, dementia, or MS. In these cases, treatment will focus on addressing the cause of the foreign accent syndrome. A doctor might prescribe medication for conditions such as MS or surgery for certain brain growths. When there is a psychiatric cause, a doctor may recommend therapy, medication, or both. Many causes of foreign accent syndrome are not curable, though medication can help manage symptoms. In most cases, a doctor will recommend speech therapy to help a person regain their normal habits. When the cause of foreign accent syndrome is unclear — such as in the case of the woman who developed it following dental surgery — speech therapy may be the only treatment option
Traumatic Brain Injury (TBI) disrupts the normal functioning of the brain due to a strike or jolt to the head. This can cause vision problems, such as blurred or double vision, and difficulty wi eye movements, focus, and tracking. This can result in headaches, dizziness and nausea— especially when someone who has suffe ed a TBI needs to retain focus on a fixed poin or task. Over 10 million TBIs occur annually around the world and around 57 million people have been hospitalized for a TBI at some point in their lives. Studies show that over 90% of Traumatic Brain Injury patients suffer some form of visua dysfunction, yet vision problems tend to be overlooked during the initial treatment of a brain injury. At times, vision problems don’t manifest until some time has passed— so make sure to pay close attention to any vision changes you may experience following a concussion or head trauma. If you notice any alterations in your vision, contact our optometrists right away. The eye doctor will determine the causes of the vision change and will provide the appropriate vision therapy treatment
Often the affected person with a TBI is not aware of their specific vision dysfunction but might complain of one or more of the signs below: Traumatic Brain Injuries tend to interrupt the communication between the eyes and the brain, which can cause a range of visual dysfunctions. The signs often include: - Blurred vision - Eyestrain - Sensitivity to light - Reading difficulti - Attention and concentration difficulti Below is a more detailed list of the common vision problems that can result from brain injury or a medical condition, such as a stroke, tumor, aneurysm, meningitis, cerebral palsy, and other neurological insults. Visual Acuity – Blurry vision, either all the time or can shift in and out of focus. Eye focusing – Inability to quickly change focus from near to far objects. Eye teaming – The eyes not working in tandem, potentially causing double vision.
Eye Movements – Difficulty following a movin object or losing one’s place while reading. Motion Sensitivity – The disruption of the connection between vision integration and balance system which makes it difficult t process motion properly. This can cause vertigo or unease when traveling, scrolling a digital device, or when in busy environments such as grocery stores, social settings, or sporting events. Visual Field Loss – The partial or complete loss of peripheral vision. Visual field loss may cause one to bump into objects, be struck by approaching objects, or experience frequent falls. Visual Memory Loss – Losing the ability to recall or remember visual information stored in long or short-term visual memory. This can have a devastating impact on daily functioning as the individual no longer recalls numbers, words, pictures, or any data viewed in the past. Reading comprehension decreases, and the ability to recognize locations and faces declines. One may not remember where a specific object—such as a car key—was put or how to give directions. Headaches or Eye Pain – Following head trauma, the individual may experience a range of headaches or even a stabbing pain around the eye — at times accompanied by redness, burning, or itching of the eyes Sensitivity to Light – In the aftermath of a brain injury, one can develop sensitivity to light and be unable to tolerate glare. Also known as photophobia, sensitivity to light can be exacerbated by particular light sources, such as bright sunlight and fluo escent lighting. LCD screens, used for computers or smartphone devices, can be particularly intolerable after a concussion. People of all ages who develop visual dysfunction due to a neurological trauma or injury can benefit f om a vision assessment by a Neuro-Optometric Rehabilitation Optometrist (neuro-optometrist). These eye care professionals are highly trained in the diagnosis, treatment and rehabilitation of neurological conditions that affec the visual system, as well as perceptual and motor disorders. Research studies show that patients having undergone a vision rehabilitation program can vastly improve their quality of life. An interdisciplinary rehabilitation team is essential for patients with concussions, strokes or other neurological deficits. In addition t optometrists, team members may include nurses, physical therapists, occupational therapists, speechlanguage pathologists, physical medicine doctors, neurologists, neuropsychologists, audiologists, and ophthalmologists, among others.
Mild or moderate COVID-19 lasts about two weeks for most people. But in some, the long-term effects of COVID-19 can cause lingering health problems and wreak havoc for months. Tae Chung, M.D., a specialist in neurology and physical medicine and rehabilitation; Megan Hosey, Ph.D., an expert in rehabilitation psychology; Arun Venkatesan, M.D., Ph.D., a specialist in neurology; Amanda Morrow, M.D., an expert in pediatric rehabilitation medicine; and Ann M. Parker, M.D., Ph.D., who specializes in lung disease and critical care, discuss long-term COVID-19, what symptoms are most common and what those affected by them can expect Mild or moderate COVID-19 lasts about two weeks for most people. But others experience lingering health problems even after the fever and cough go away and they are no longer testing positive for the illness.
Parker notes that the World Health Organization has developed a definition for post-COVID-19 condition (the WHO’s term for long COVID) as coronavirus symptoms that persist or return three months after a person becomes ill from infection with SARS CoV-2, the coronavirus that causes COVID-19. Those symptoms can include fatigue, shortness of breath and cognitive problems. The symptoms can come and go, but have an impact on the person’s everyday functioning, and cannot be explained by another health problem. WHAT CAUSES POST-COVID SYNDROME? While it’s clear that people with certain risk factors (including high blood pressure, smoking, diabetes, obesity and other conditions) are more likely to have a serious bout of COVID-19, there isn’t a clear link between these risk factors and long-term problems. In fact, long COVID can happen in people who have mild symptoms, although patients with more severe initial illness seem to be more likely to have long-term impairments.
More studies will shed light on why these stubborn health problems persist in some people. SARS-CoV-2 can attack the body in a range of ways, causing damage to the lungs, heart, nervous system, kidneys, liver and other organs. Mental health problems can arise from grief and loss, unresolved pain or fatigue, or from post-traumatic stress disorder (PTSD) after treatment in the intensive care unit (ICU).
Doctors are seeing a spectrum of symptoms after acute COVID-19, some of which would be expected after other critical illnesses. Some are minor, but other people may need continuing care and even readmission to the hospital. Similar, lingering problems can affect patients with other serious illnesses. But it is notable that post-COVID-19 syndrome is not just afflicting people who were very sick with the coronavirus: Some patients who were never severely ill with COVID-19 are experiencing long-term symptoms.
DO COVID VACCINES PREVENT LONG COVID?
Getting vaccinated for COVID-19 lowers the risks of COVID infection. While breakthrough infections are possible, being fully vaccinated and boosted is effective in reducing the risk of hospitalization and death due to COVID. Research is ongoing about how long COVID affects people who had breakthrough COVID, but it is likely that being vaccinated reduces the risk.
POST-COVID SYNDROME CONDITIONS
The senses of smell and taste are related, and because the coronavirus can affect cells in the nose, having COVID-19 can result in lost or distorted senses of smell (anosmia) or taste. Before and after people become ill with COVID-19, they might lose their sense of smell or taste entirely, or find that familiar things smell or taste bad, strange or different. For about a quarter of people with COVID-19 who have one or both of these symptoms, the problem resolves in a couple of weeks. But for most, these symptoms persist. Though not life-threatening, prolonged distortion of these senses can be devastating and can lead to lack of appetite, anxiety and depression. Some studies suggest that there’s a 60% to 80% chance that these people will see improvement in their sense of smell within a year. Neurologist Arun Venkatesan, M.D., Ph.D., says, “Some individuals develop medium to long-term symptoms following COVID infection, including brain fog, fatigue, headaches and dizziness. The cause of these symptoms is unclear but is an active area of investigation
Can COVID-19 increase a person’s risk for anxiety, depression and cognitive issues? A study of COVID-19’s impact on mental and emotional well-being conducted by Johns Hopkins experts in psychiatry, cognition (thinking, reasoning and remembering) and mental health found that these problems were common among a diverse sample of COVID-19 survivors. Cognitive impairment after acute coronavirus infection can have a severe impact on a person’s life. Long-haul COVID patients may experience changes in the way they think, concentrate, speak and remember, and these symptoms can affect their ability to work or even maintain activities of daily living. After recovering from the coronavirus, some people are left with lingering anxiety, depression and other post-COVID mental health issues.
Physical changes such as pain and weakness can be complicated by long periods of isolation, stress from job loss and financial difficulties, and grief from the deaths of loved ones and the loss of good health. The relationship between COVID-19 and diabetes, especially type 2 diabetes, is complex. Type 2 diabetes is a risk factor for serious cases of COVID-19, and some survivors of the illness seem to be developing type 2 diabetes signs after they recover from COVID-19. It’s not yet known whether children who have had COVID-19 are more or less likely than adults to experience continuing symptoms. But long-term COVID-19 in children is a possibility, showing up as fatigue, headaches, difficulty with school work, mood concerns, shortness of breath and other long-hauler symptoms.
SEVERE POST-COVID COSTOCHONDRITIS
Although children comprise the fewest cases of COVID-19 infection, symptoms and complications among the various age groups affected, new long-term consequences a e being reported including severe costochondritis. Post-COVID costochondritis (PCC) is an inflammation of the cartilage that connects a rib to the breastbone. The syndrome causes pain and tenderness on the breastbone, pain in more than one rib, or pain that gets worse with deep breaths or coughing. Patients will experience sharp or aching pain which can start suddenly or develop slowly and spread across the chest. Because of the location of the pain, the symptoms are sometimes misinterpreted as a heart attack. Costochondritis usually goes away on its own, although it might last for several weeks or longer. Treatment focuses on pain relief with traditional treatments including injections to relieve pain and medications — though PCC, in many cases, is unresonsive to these treatments. Physical therapy in the form of gentle stretching exercises for the chest muscles might be helpful. Medications used to treat PCC may include nonsteroidal anti-inflammatory d ugs. Some of these drugs, such as ibuprofen
(Advil, Motrin IB) or naproxen sodium (Aleve), can be purchased over the counter. Stronger versions are available by prescription. Side effects of these medicines can include damage to th stomach lining and kidneys. Narcotics may also be used if pain is severe, however, are avoided when possible because they can be habit-forming. Antidepressants such as amitriptyline are often used to control chronic pain — especially if the pain interferes with sleep and anti-seizure medication such as gabapentin (Gralise, Neurontin) has also proved successful in controlling chronic pain caused by PCC. In a study conducted at the School of Medicine, Texas Tech University Health Sciences Center in Lubbock, Texas, researchers found that PCC in some cases may respond to treatment with colchicine, an anti-inflammator . Another option is a procedure called transcutaneous electrical nerve stimulation (TENS), in which a device sends a weak electrical current via adhesive patches on the skin near the area of pain. The current is thought to possibly interrupt pain signals, preventing them from reaching the brain. If conservative measures are not successful, the injection of numbing medication and a corticosteroid directly into the painful joint is also an option.


CARDIOVASCULAR CONDITIONS
A study published in Nature Medicine by researchers at the Veterans Affairs ( A) St Louis Health Care System, found that in the year after recovering from the illness’s acute phase, patients had increased risks of an array of cardiovascular problems, including abnormal heart rhythms, heart muscle inflammation, blood clots, st okes, myocardial infarction, and heart failure. What’s more, the heightened risks were evident even among those who weren’t hospitalized with acute COVID-19. Patients with more severe disease—determined by whether they recuperated at home, were hospitalized, or were admitted to the intensive care unit—had higher risks. But the risks were evident even among those who were not hospitalized with COVID-19. Other subgroup analysis found increased risks regardless of age, race, sex, obesity, smoking, hypertension, diabetes, chronic kidney disease, hyperlipidemia and preexisting cardiovascular disease.
RESPIRATORY ISSUES
Severe cases of COVID-19 can produce scarring and other permanent problems in the lungs. This is likely due to a combination of the body’s exaggerated immune system reaction to the virus, and the lung inflammation it triggers. Even mil infections can result in persistent respirtory distress — causing shortness of breath after even light exertion. Lung recovery after COVID-19 is possible, but takes time. Experts say it can take months for a person’s lung function to return to pre-COVID-19 levels. Breathing exercises and respiratory therapy can help. Researchers from the University of Iowa recently conducted a study to understand the long-term effects of COVID-19 on lun function. The study enrolled 100 adults with a confirmed SARS CoV-2 infection who remained symptomatic for more than 30 days following the diagnosis, with a control group of 106 healthy participants. The results provided evidence of airway damage many months after the initial SARS CoV-2 infection.
CHRONIC FATIGUE
A team of researchers, including two from Johns Hopkins Medicine, have published a review article highlighting similarities between certain lingering symptoms following COVID-19 illness — a condition called “long COVID” — and myalgic encephalomyelitis/chronic fatigue syndrome (ME/ CFS), a debilitating, complex disorder previously known as chronic fatigue syndrome. The researchers say the symptoms shared by the two conditions may involve a biological response that goes haywire when the body encounters certain infections or other environmental hazards. “The body’s response to infection and injury is complex and covers all body systems,” says the study’s lead author Bindu Paul, Ph.D., assistant professor of pharmacology and molecular sciences at the Johns Hopkins University School of Medicine. “When that response is in disarray — even just one aspect of it — it can cause feelings of being tired, brain fog, pain and other symptoms.”
LOSS OF TASTE AND SMELL
The senses of smell and taste are related, and because the coronavirus can affect cells in the nose, having COVID-19 can result in lost or distorted senses of smell (anosmia) or taste. Before and after people become ill with COVID-19, they might lose their sense of smell or taste entirely, or find that familiar things smell or taste bad, strange or diffe ent. For about a quarter of people with COVID-19 who have one or both of these symptoms, the problem resolves in a couple of weeks. But for most, these symptoms persist. Though not life-threatening, prolonged distortion of these senses can be devastating and can lead to lack of appetite, anxiety and depression. Some studies suggest that there’s a 60% to 80% chance that these people will see improvement in their sense of smell within a year
MUSCULOSKELETAL CONDITIONS
Recent studies have suggested that musculoskeletal symptoms, including joint and muscle pain, are present in many COVID-19 patients after the acute phase of infection, persisting for weeks or even months after the initial infection. Comprising 40% of the human body weight, the skeletal muscle is an important organized tissue composed by numerous bundles of myofibers. It has a crucial mechanical role, generating force and power through the conversion of chemical to mechanical energy, which yields movement, facilitating our daily activities. Furthermore, skeletal muscle can store energetic substrates (carbohydrates and amino acids) for the basal metabolism and it can contribute to heat production, stabilizing the body’s temperature. Considering the multiple functions of the musculoskeletal system and the fact that COVID-19 is a multi-organic disease, it isn’t surprising that musculoskeletal issues may arrise from infection.
SLEEP DISORDERS
“Sleep disorders are one of the most common symptoms for patients who’ve had COVID-19,” says sleep medicine specialist Cinthya Pena Orbea, MD. “They report insomnia, fatigue, brain fog and sometimes we even see circadian rhythm disorders.” Coined “coronasomnia,” COVID-19- induced insomnia is often attributed to pandemic-related stress, anxiety, depression and other mental health conditions. According to Dr. Orbea, many people have a delayed sleep cycle, causing them to fall asleep much later in the evening or earlier in the morning. This delayed cycle extends into the following day, causing people to feel groggy, have chronic fatigue or wake up later than they prefer. “Sleep is extremely important for the overall function of our bodies, including our metabolic systems and our immune systems,” explains Dr. Orbea. “Since sleep is important for concentration and memory function, it will enhance how patients recover from the disease and impact their quality of life.” During illness, the immune system’s response to an infection can have a profound effect on sleep. Likewise, getting adequate, good quality sleep is crucial for your immune system to work optimally. In long COVID, if the immune system is still not functioning normally, the body will be constantly trying its hardest to reduce the inflammation. This could explain why so many people with long COVID report fatigue and sleep difficulties as major symptoms. It’ also thought that inflammation can come and go during long COVID, which would mean that the body is constantly having to work to keep everything in balance. When the body is having to deal with chronic inflammation, sleep can be reduced and sleep quality can be compromised.
PERIPHERAL NEUROPATHY
Some patients with long COVID may have long-lasting nerve damage resulting in weakness, numbness and pain, usually in the hands and feet. This condition , known as peripheral neuropathy, appears to be caused by immunity problems triggered by infection according to a new study published in the journal Neurology: Neuroimmunology & Neuroinflammation. “This is one of the early papers looking into causes of long COVID, which will steadily increase in importance as acute COVID wanes,” said Anne Louise Oaklander, MD, the lead study author and a neurologist at Massachusetts General Hospital. “Our findings suggest that some long COVID patients had damage to their peripheral nerve fibers and that damage to the small-fiber type of nerve cell may be prominent.” The study found that 10 patients — or 59% — had at least one test that confirmed neuropathy. Two patients had rare neuropathies that affected muscle nerves and 10 were diagnosed with small-fiber neuropathy, which is a cause of chronic pain. Common symptoms included fatigue, weakness, changes in their senses, and pain in their hands and feet.

COGNITIVE DEFICITS
Post COVID neurological problems have been commonly reported and include cognitive or memory disturbances, headache and myalgia. Acute neurological diagnoses include encephalopathy, delirium, cerebrovascular disease, seizures, neuropathy and myopathy. Less frequently reported problems include abnormal movements, psychomotor agitation, syncope and autonomic dysfunction. Another common complaint amongst post COVID patients is brain fog, a term used to describe slow or sluggish thinking. Brain fog can occur under many different circumstances — for example, when someone is sleep-deprived or feeling unwell, or due to side effects from medicines that cause drowsiness. Brain fog can also occur following chemotherapy or a concussion. In many cases, brain fog is temporary and gets better on its own. However, we don’t really understand why brain fog happens after COVID-19, or how long these symptoms are likely to last. But we do know that this form of brain fog can affect different aspects of cognition.
Among patients hospitalized with COVID-19, 1 year after discharge, about half experienced clinically relevant moderate or worse diminished cognitive ability in verbal learning and executive function, according to study findings published in European Neuropsychopharmacology. Lingering cognitive, neurologic, psychiatric, and physical symptoms after COVID are estimated to affect as many as 40 of all patients who contracted COVID-19 and as much as 85% of those who have been hospitalized with COVID-19. Cognitive COVID (which is long-term) is characterized by brain fog, and memory and concentration struggles, and is recognizable in about 30% of patients previously hospitalized with the virus. COVID infection frequently leads to brain damage — particularly in those over 70. While sometimes the brain damage is obvious and leads to major cognitive impairment, more frequently the damage is mild, leading to difficulties with sustained atte ion. Although many people who have recovered from COVID can resume their daily lives without difficulty — even if they ha some deficits in attention — the e are a number of people who may experience difficulty for an extended period
Diagnosing TBI can be complicated. Currently, doctors use a variety of methods to determine if a patient has a TBI. A medical exam is the first step to diagnose a potential brain injury which includes a neurological exam. This exam evaluates thinking motor function, sensory function, coordination, eye movement, and reflexes. Although it is well acknowledged within the medical community that they can not detect TBIs, CT and MRI scans are typically the next step because they can rule out a more serious brain injury. Although these protocols aid health care providers who are trained in the intricacies of diagnosing TBIs, none on their own can provide a definitive diagnosis. However, there is promising research showing that more advanced imaging may take center stage in the diagnosis of both TBI and mTBI (mild traumatic brain injury).
This next-level imaging falls into two categories: Nuclear Medicine in the form of single-photon emission computerized tomography (SPECT) and positron emission tomography (PET) scans and Diffusion Tensor Imaging (DTI) scans.
SPECT AND PET SCANS
SPECT is a nuclear imaging scan that integrates computed tomography (CT) and a radioactive tracer. The tracer is what allows doctors to see how blood flows to brain tissue. Before the SPECT scan, a tracer is injected into your bloodstream. The tracer is radiolabeled, meaning it emits gamma rays that can be detected by the CT scanner. The computer collects the information emitted by the gamma rays and displays it on the CT cross-sections. These cross-sections can be added back together to form a 3D image of your brain. The radioactive tracers will pass through your body and be detected by the scanner.
PET scans also use radiotracers however for additional purposes other than monitoring blood flow. PET scans also visualize and measure and physiological processes such as regional chemical composition and absorption. In both SPECT and PET scans, different tracers are used depending on the purpose of the scan. In the case of TBI screening, Fluorodeoxyglucose (FDG) is the most widely used radiotracer.
A SPECT scan differs from a PET scan in that with SPECT the tracer stays in your bloodstream rather than being absorbed by surrounding tissues, thereby limiting the images to areas where blood flows. SPECT scans are cheaper and more readily available than higher resolution PET scans, though both scans can detect minute molecular biological changes in the brain, which is not possible for MRI or CT scans.
According to Dr. Daniel Amen, a brain health expert, “Brain SPECT imaging identifies areas of the brain hurt by TBI. CT and MRI scans show if there is any damage to the anatomy or structure of your brain, but these scans cannot tell how your brain is functioning. In fact, after a TBI, CT or MRI scans will often appear normal when there is actually functional damage to the brain that can be detected with SPECT.”
DTI SCAN
DTI scans are a relatively new magnetic resonance imaging (MRI) technique that is used to evaluate microstructural changes in the brain by measuring water molecules in tissue. Its imaging capabilities are based on the ability to determine the orientation and diffusion characteristics of white matter. Recent advances in the resolution of DTI have made it possible to visualize potential changes in various neural tracts associated with brain injury. DTI is used in conjunction with conventional MRI techniques to provide 2-dimensional and 3-dimensional visualization of changes to white matter in the brain. DTI scans can provide image contrast that was previously unattainable using conventional MRI techniques.
According to Lauren J. O’Donnell, PhD of the Golby Neurosurgical Brain Mapping Laboratory, DTI is a sensitive probe of cellular structure that works by measuring the diffusion of water molecules. Unlike the diffusion in a glass of pure water, which would be the same in all directions (isotropic), the diffusion measured in tissue varies with direction (is anisotropic). The measured macroscopic diffusion anisotropy is due to microscopic tissue heterogeneity. In the white matter of the brain, diffusion anisotropy is primarily caused by cellular membranes, with some contribution from myelination and the packing of the axons. Anisotropic diffusion can indicate the underlying tissue orientation.
WHAT ADVANCED IMAGING TECHNIQUES MEAN FOR TBI PATIENTS
Being able to thrive with TBI means getting the proper diagnosis, which is the first step in getting the appropriate treatment. SPECT, PET, and DTI scans are making this possible for more patients. The amount of detail and diagnostic information made available by these scans can help doctors create very customized treatment plans for patients with TBI.
With more research being done every year to develop advanced imaging modalities, the future is definitely brighter for patients suffering from TBI.
Chronic Traumatic Encephalopathy (CTE) is a progressive degenerative disease of the brain found in people with a history of repetitive brain trauma. CTE affects athletes who participate in sports which expose them to repeated head trauma such as boxing, football, and hockey. Military veterans are also at risk, with military service carrying a high potential for head trauma in many cases.
Football in particular has gained a lot of attention around CTE. “You are supposed to be tough. You are supposed to play through pain. You are not supposed to cry. We are taught that early on in the game as kids. Tough sport. Brutal sport. It’s like being a gladiator. People want to see the big hits. And as a player, you don’t want to admit you are injured.” says Hall of Fame running back Eric Dickerson.
Patients can present with symptoms of CTE many years after head trauma has occurred. This is possible because repeated brain trauma triggers a slow progression of brain tissue degeneration. These changes in the brain can begin months, years, or even decades after the last brain trauma has occurred.
SYMPTOMS OF CTE AND DIAGNOSIS
The symptoms of CTE can mimic dementia, even being called ‘dementia pugilistic’ when it was first discovered. May scientists disagree on the symptoms of CTE and research is still underway, however, the disease has been associated with memory and thinking problems, confusion, personality changes, and/or erratic behavior including aggression, depression, and even suicidal thinking. Other symptoms may include problems paying attention and organizing thoughts as well as difficulty with balance and motor skills.
CTE eludes diagnosis due to symptom overlap with other brain disorders such as Alzheimer’s disease and Parkinson’s disease and also psychiatric disorders such as clinical depression. Because of the commonalities between CTE and these disorders, a CTE diagnosis can only be made after death, when an autopsy can reveal whether the known brain changes of CTE are present. That being said, when CTE is suspected, neurological testing and psychiatric screening can be used to rule out other issues
THE SILENT KILLER
Even when concussions are asymptomatic, they can still contribute to brain degeneration, making CTE a silent killer. The culprit in this degeneration is an abnormal protein call tau. Tau is also associated with dementia, however, research has found that with CTE a unique pattern of abnormal tau is present which builds up in the tissues and around the blood vessels.
“The question is whether, even after they are asymptomatic, players might still be recovering in ways we don’t know much about. It has shown that up to 3 or 4 weeks after concussion and the disappearance of symptoms, there are subtle differences in brain activity—suggesting recovery may not be complete. This is the stuff that nags at any doctor making return-to-play decisions.” says Dr. Robert Cantu, Professor of Neurosurgery at Boston University Medical School and Co-Director of the Center for the Study of Traumatic Encephalopathy (CTE).
THE SCIENCE BEHIND THE PATHOLOGY
To understand the science behind CTE, you first need to understand its different stages. In stage one, symptoms are fairly mild and can include headaches as well as loss of attention and concentration. The physical characteristics of a brain with stage one CTE are unremarkable and sometimes nonexistent — approximately one-half of brains with stage one CTE show visible pathology. When present, they are only microscopically detectable and most commonly localized to the frontal, temporal, insular, septal, and parietal areas of the brain.
In stage two, CTE can present with symptoms of depression or mood swings, explosively and short-term memory loss, in addition to stage one symptoms. Less common stage two symptoms can include executive dysfunction, language difficulties, and impulsivity. The physical characteristics of a brain with stage two CTE are more prominent than in stage one and include mind enlargement of the frontal ventricles as well as other areas of the brain. In addition, detectable levels of tau protein are present in the frontal and temporal areas of the brain. Also present in the brain are pre-neurofibrillary tangles (NFTs) which are aggregates of tau protein.
In stages three and four, the most advanced stages of CTE, patients exhibit all of the symptoms of the first two stages however the severity of symptoms is drastically increased. At stage three 75% of patients are considered cognitively impaired. At stage four, researchers found that most patients developed a profound loss of attention and concentration, executive dysfunction, language difficulties, explosivity, aggressive tendencies, paranoia, depression, gait, and visuospatial difficulties.
Studies of patients in stage four also site that the most common causes of death for those with CTE are respiratory failure, cardiac disease, suicide, overdose, and symptoms associated with end-stage dementia and malignancy.
In the latter stages of CTE, the brain shows macroscopic changes with structural changes becoming evident in stage four. In the final stage of CTE, there is a reduction in brain weight, mild frontal and temporal atrophy, and enlargement of the lateral and third ventricles. The presence of NFTs becomes prevalent as well, showing up both superficially and deep within the brain. In short, the entire brain becomes overtaken with pathology.
RESEARCH AND TREATMENT
Millions of dollars are being invested in CTE research by organizations such as the National Institute of Neurological Disorders and Stroke and Brain Injury Research Institute and the Alzheimer’s Association. As a result, better imaging techniques are becoming available and there is hope that in the future CTE will be diagnosable before death. This will inevitably bring forth treatment options for patients suffering from CTE. There is currently no cure or treatment for the disease which makes this research very important for the numerous people suffering from the disease’s effects.
SOURCE UNIVERSITY OF GEORGIA
In a new study at the University of Georgia, researchers have demonstrated the long-term benefits of a hydrogel, which they call ‘brain glue,’ for the treatment of traumatic brain injury. The gel protects against loss of brain tissue after a severe injury and might aid in functional neural repair.
The study shows the long-term benefits of a hydrogel, or “brain glue,” for the treatment of traumatic brain injury. The new study provides evidence that not only does the gel protect against loss of brain tissue after a severe injury, but it also might aid in functional neural repair. Brain damage following significant TBI commonly results in extensive tissue loss and long-term disability. There currently are no clinical treatments to prevent the resulting cognitive impairments or tissue loss. As reported in Sciences Advances, the new finding is the first to provide visual and functional evidence of the repair of brain neural circuits involved in the reach-to-grasp movement in brain glue-implanted animals following severe TBI.
“Our work provides a holistic view of what’s going on in the recovery of the damaged region while the animal is accomplishing a specific reach-and-grasp task,” said lead investigator Lohitash Karumbaiah, an associate professor in the University of Georgia’s College of Agricultural and Environmental Sciences.
Brain glue was designed to mimic the structure and function of the meshwork of sugars that support brain cells. The gel contains key structures that bind to basic fibroblast growth factors and brain-derived neurotrophic factors, two protective protein factors that can enhance the survival and regrowth of brain cells after severe TBI.
In a prior short-term study, Karumbaiah and his team showed that brain glue significantly protected brain tissue from severe TBI damage. In this new research, to harness the neuroprotective capacity of the original, they further engineered the delivery surface of protective factors to help accelerate the regeneration and functional activity of brain cells. After 10 weeks, the results were apparent.
“Animal subjects that were implanted with the brain glue actually showed repair of severely damaged tissue of the brain,” said Karumbaiah. “The animals also elicited a quicker recovery time compared to subjects without these materials.”
To measure the glue’s effectiveness, the team used a tissue-clearing method to make brain tissue optically transparent, which allowed them to visually capture the immediate response of cells in the reach-to-grasp circuit using a 3D imaging technique.
BY NAOMI KHAN
Hyperbaric oxygen therapy (HBOT) is defined as the use of oxygen at higher than atmospheric pressure for the treatment of underlying disease processes and the diseases they produce. Modern HBOT in which 100% O2 is breathed in a pressurized chamber dates back to the 1930s when it was first used for the treatment of decompression illness in divers. There are currently 13 FDA-approved uses for HBOT.
Though TBI treatment is not an FDA-approved use for HBOT, many physicians have used it as an “off-label” treatment with notable results. Though not yet scientifically proven, it has been said that HBOT can dramatically and permanently improve symptoms of chronic TBI months or even many years after trauma. This assertion is generally met with skepticism within the medical establishment because it is widely accepted that any post-concussion symptoms persisting more than 6 months after a head injury is due to permanent brain damage that cannot be repaired. Therefore, treatment has been limited to symptom management and rehabilitative services, and any claim suggesting that fundamental healing is possible is not considered mainstream.
Researchers started investigating HBOT as a TBI treatment in the 1960s because of its ability to slow cell death, suppress inflammation, and boost cell and blood vessel growth. Most of the research was conducted on animals until recently because of the ethical issues involved in experimenting on humans with acute, severe brain injury.
One of the biggest issues complicating research of HBOT in brain injury is the ability to conduct randomized, double-blind, placebo-controlled studies. Brain injury varies widely from person to person, making it difficult to find TBI patients to study who have similar injury severity and affected regions.
Finding an objective way to measure the effects of HBOT is also an obstacle with several published studies failing to use a placebo. However, recently researchers have devised and used a placebo for HBOT in their studies, usually by increasing the air pressure without changing the oxygen content of the air being delivered. It’s imperfect (since air pressure increases while oxygen stays the same), but it does improve the reliability of results and possibly paves the way for HBOT as an acknowledged treatment for TBI.
Contribute to the TBI Times