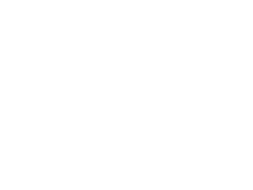
Traumatic brain injury (tbi) is a major concern in both medical and military fields, affecting millions of people worldwide. The impact on brain function may range from mild concussions to severe, life-altering damage. Traditional treatments, such as physical therapy and medication, often address symptoms but may not fully promote brain healing. However, recent studies suggest that ketamine therapy could be an innovative approach in helping patients with TBI recover.
Ketamine is a dissociative anesthetic that has been used for decades in surgical settings. Its ability to block N-methyl-D-aspartate (NMDA) receptors in the brain gives it unique properties, particularly in its ability to induce anesthesia without affecting breathing or heart function. More recently, ketamine has gained attention for its therapeutic potential in treating depression, post-traumatic stress disorder
(PTSD), chronic pain and, as of recent studies, TBI.
TBI may lead to a range of cognitive, emotional and physical impairments due to neuronal damage and inflammation. Ketamine therapy is believed to aid in recovery through several mechanisms:
Neuroplasticity Promotion: One of the most exciting aspects of ketamine’s potential for TBI treatment is its ability to enhance neuroplasticity — the brain’s capacity to reorganize itself by forming new neural connections. This is especially critical after a TBI, where damaged brain cells need to be repaired or replaced. Ketamine has been shown to stimulate the release of brain-derived neurotrophic factor (BDNF), a protein essential for neuron growth and survival.
Reduction of Inflammation: Following a brain injury, inflammation is a significant contributor to secondary brain damage. Ketamine has anti-inflammatory properties that may help reduce the extent of this damage, protecting brain tissue from further harm and supporting recovery.
Glutamate Regulation: Ketamine works by blocking NMDA receptors involved in glutamate signaling. Glutamate is a neurotransmitter crucial for memory and learning but can be neurotoxic in excess. By regulating glutamate levels, ketamine helps prevent further neuronal injury and promotes healthy brain function.
Mood and Cognitive Improvement: TBI patients often experience depression, anxiety and cognitive impairments. Ketamine’s rapid antidepressant effects can improve mood and enhance cognitive function, creating an optimal environment for rehabilitation therapies to be more effective.
While more research is needed to fully understand the scope of ketamine’s benefits for TBI patients, early findings suggest that it could be a breakthrough in brain injury treatment. By promoting neuroplasticity, reducing inflammation and improving mood, ketamine therapy offers hope for those recovering from TBI. As clinical trials progress, ketamine may become an integral part of TBI rehabilitation strategies, providing a new lifeline for patients seeking recovery.
Stephen casper, ph.D., A noted medical historian, offers a critical examination of the rise and decline of recognition of chronic traumatic encephalopathy (CTE) in the context of professional sports. His argument revolves around a paradox: while CTE was once widely acknowledged as a significant danger to athletes, its growing recognition as a problem has led to a dangerous trend where it is increasingly dismissed or ignored, especially in contact sports like football, boxing and hockey.
THE HISTORY OF CTE AWARENESS
Casper’s analysis begins with the origins of CTE as a medical concept. The condition itself, first identified in the 1920s, was initially associated with boxers who suffered from repeated head trauma. In those early days, the condition was known as “punch-drunk syndrome,” a term that was commonly used in the medical community. As research evolved, it became clear that repetitive head trauma in various sports led to a range of cognitive and psychological symptoms, including memory loss, aggression and depression.

Left: A normal, healthy brain. Right: A brain with advanced CTE.
In the latter half of the 20th century, this growing body of evidence led to a broader understanding of CTE. The 1990s and 2000s saw some mainstream attention to the condition, particularly as athletes began to come forward with their stories. For instance, the death of former NFL players, such as Mike Webster, raised questions about the long-term impacts of repetitive head injuries. Posthumous examinations of their brains revealed patterns of degeneration that were consistent with CTE.
For a time, the presence of CTE in athletes was widely acknowledged in both academic circles and the general public. Medical professionals and former athletes began to advocate for reforms in contact sports to limit the risk of head trauma, and there was a growing consensus that something needed to be done to protect players.
THE DECLINE OF RECOGNITION IN PROFESSIONAL SPORTS
Casper argues that, despite the earlier recognition of the dangers of CTE, there has been a troubling shift in professional sports. While CTE remains a central issue in academic and medical research, the sports industry itself has begun to downplay or ignore its potential dangers. This shift can be traced to a few key factors.

THE ECONOMIC AND CULTURAL INTERESTS OF PROFESSIONAL SPORTS
At the heart of this change is the immense financial and cultural power of professional sports. In leagues like the NFL, the NHL and other contact sports organizations, the revenue generated from games, sponsorships and media deals is enormous. The idea of reforming the way the sport is played — or worse, changing the very nature of the game — may be seen as a threat to the financial model that underpins the entire industry.
The resistance to acknowledging CTE’s long-term effects can, therefore, be understood in the context of these powerful economic interests. For instance, while the NFL has faced growing scrutiny for its role in the CTE crisis, the organization has been accused of downplaying the issue, often by funding studies that cast doubt on the extent of the damage caused by head injuries. This has contributed to a culture in which the real dangers of CTE are minimized in favor of maintaining the status quo.
THE PSYCHOLOGICAL DENIAL AMONG ATHLETES
Another contributing factor, according to Casper, is the psychology of professional athletes themselves. Many athletes are deeply invested in the idea of toughness and the willingness to push through pain. In contact sports, there is a long-standing culture of “playing through the pain,” and athletes often view injury as a part of their job, rather than a potential threat to their future well-being. This mindset has led many athletes to dismiss or downplay the risks of CTE, particularly when faced with the potential of their career coming to an end due to health concerns.
Michael Lewis Webster, who died with CTE, was an American football center in the National Football League from 1974 to 1990 with the Pittsburgh Steelers and Kansas City Chiefs. He is a member of the Pro Football Hall of Fame, class of 1997.
Furthermore, there is a significant stigma surrounding mental health in the athletic world, especially among men. Admitting to problems like memory loss, depression, or aggression may be seen as a sign of weakness. The refusal to acknowledge CTE symptoms, therefore, can be understood as a form of self-preservation, as athletes try to maintain their image and identity as invulnerable competitors.

Tiaina Baul “Junior” Seau Jr., who suffers from CTE, was an American professional football linebacker who played in the National Football League, mostly with the San Diego Chargers. Known for his passionate play, he was a 6-time first-team All-Pro, 12-time Pro Bowl selection and named to the NFL 1990s All-Decade Team.
THE ROLE OF MEDICAL EXPERTS AND MEDIA
Casper also critiques the role of the media and medical experts in contributing to the marginalization of CTE. In the early 2000s, when CTE research began to gain attention, the media played an important role in spreading awareness about the condition. However, as the issue became more contentious, some media outlets began to back away from the narrative. Partly due to pressure from sports organizations, the portrayal of CTE began to shift from an established concern to a more disputed topic.
In the case of the NFL, a notable instance of this shift was the release of the movie “Concussion” in 2015, which dramatized the story of Dr. Bennet Omalu, the forensic pathologist who first discovered CTE in football players. The NFL’s response to the film and its portrayal of CTE was one of aggressive denial, leading to public confusion over the true extent of the issue. Some medical professionals also became less willing to engage with the topic of CTE directly, choosing to focus on less controversial topics or minimizing the long-term risks associated with repetitive head trauma.
THE ONGOING PROBLEM: A CALL FOR REFORMS
Despite efforts to downplay the issue, there is still significant concern about the long-term consequences of CTE for athletes. Casper’s work urges a return to a more honest, scientific discussion of the risks posed by contact sports, advocating for reforms such as rule changes to limit head trauma, better concussion protocols and greater education on long-term effects. Moreover, Casper believes the sports industry must move away from denial regarding CTE, prioritizing athletes’ health over the financial interests of leagues and teams. This shift is essential to ensuring athletes’ safety and reducing future cases of CTE.
IN CONCLUSION
Stephen Casper’s work highlights the disturbing trend of CTE’s growing invisibility in professional sports. What was once a widely acknowledged danger has now been relegated to the margins, largely ignored by powerful sports organizations, athletes and media outlets. Casper calls for a return to a serious, evidence-based discussion on CTE, one that prioritizes athletes’ health over economic and cultural forces that downplay head trauma risks. His argument serves as a critical reminder that the fight to protect athletes from CTE is not over and the risks must not be ignored in the pursuit of entertainment and profit.
DREAMING IS A COMPLEX AND MYSTERIOUS ASPECT OF human consciousness, with dreams offering a window into our unconscious mind. While the exact functions of dreams remain elusive, they are considered essential for emotional processing, memory consolidation and even problem-solving. However, when it comes to traumatic brain injury (TBI), the effects on dreaming are not well understood. TBI, which occurs due to an external force to the head, can cause a range of cognitive, emotional and physical impairments. It can also have a profound impact on the dreaming process, which is intricately tied to the brain’s ability to function. This article explores how TBI affects dreaming, the changes in dream patterns and the potential reasons behind these alterations.
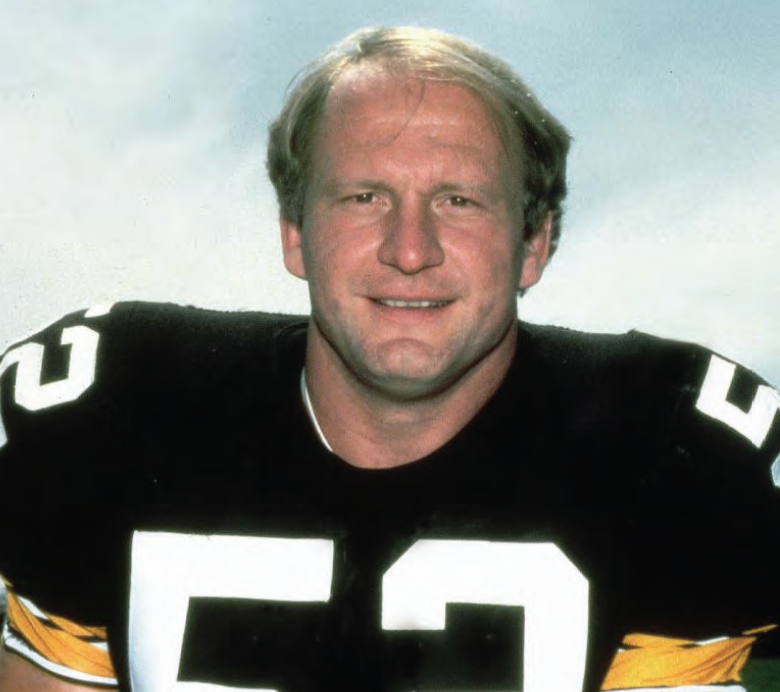
Sleep stages graph (hypnogram) above shows the different stages of sleep of participants during their session.
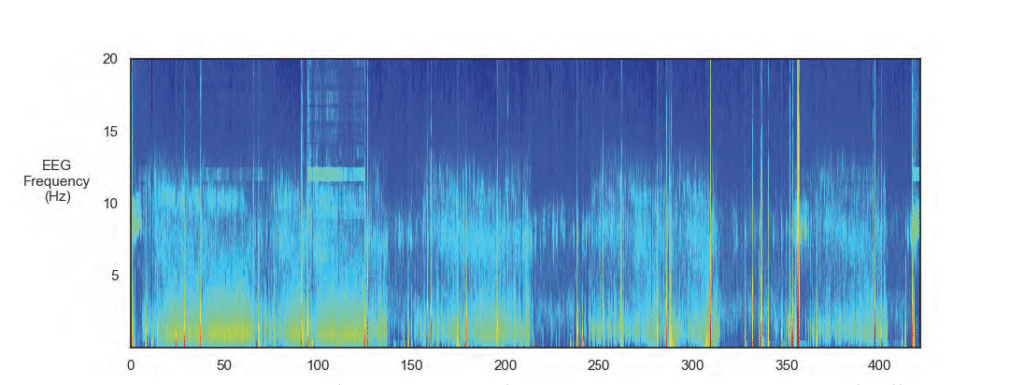
The EEG spectogram image above shows the intensity of brainwave activity over time. High-intensity regions are indicated by tones of red, yellow and green, and low-intensity regions are indicated by tones of blue.
UNDERSTANDING DREAMING AND THE BRAIN
Dreams are primarily associated with rapid eye movement (REM) sleep, a stage of sleep that is crucial for restorative processes in the brain. During REM sleep, brain activity is high, and the brain undergoes various functions, including the processing and consolidation of memories. It is during REM sleep that vivid and often surreal dreams occur. Non-REM sleep stages, especially deep sleep, also play a role in memory consolidation, physical restoration and the maintenance of cognitive functions.
The brain structures that play an essential role in dreaming include the prefrontal cortex, the limbic system (which controls emotions) and the hippocampus (which is involved in memory formation). These regions work together to create the vivid scenarios that we experience while dreaming. Traumatic brain injury can disrupt these brain structures, resulting in changes to the dreaming process, affecting both the content and quality of dreams.
THE IMPACT OF TBI ON DREAMING
The effect of TBI on dreaming varies depending on the severity of the injury, the regions of the brain affected and whether the individual is recovering from the injury. However, several common trends have emerged in research that help to explain the link between TBI and changes in dreaming.
Disruption in REM Sleep
One of the primary effects of TBI on dreaming is a disruption of the sleep cycle, especially REM sleep. Many individuals with TBI report experiencing difficulty entering or maintaining REM sleep, which in turn affects the intensity and frequency of dreams. Some individuals with TBI may experience less REM sleep overall, which reduces the opportunity for dreaming. On the other hand, some individuals report fragmented or disrupted REM sleep, leading to sleep disturbances that may cause nightmares or vivid dreams.
The disturbance in REM sleep following TBI is often linked to the brain’s inability to regulate sleep cycles effectively. Damage to brain regions such as the hypothalamus, which controls the circadian rhythm, and the brainstem, which regulates REM sleep, can result in sleep fragmentation and other disturbances that affect dreaming.
Changes in Dream Content
The content of dreams can be profoundly altered after a traumatic brain injury. Dreams may become more bizarre, fragmented or distressing. Some individuals with TBI report an increase in violent or frightening dreams, including nightmares, possibly due to heightened emotional responses to stress or trauma experienced during the injury. The emotional part of the brain, particularly the amygdala, may be affected by TBI, which could make emotions such as fear, anxiety and anger more dominant in dreams.
Moreover, people with TBI may experience more frequent dreams that revolve around the injury itself or the events surrounding it. These types of dreams may be related to post-traumatic stress, a common condition following a TBI. Dreams may replay the traumatic incident or present variations of the injury experience, leading to increased distress and anxiety. Such dreams are often reflective of the brain’s attempt to process and integrate traumatic memories.
Sleep Apnea and Other Sleep Disorders
Sleep disorders, including sleep apnea, are common in individuals with TBI. Sleep apnea is a condition in which a person’s breathing repeatedly stops and starts during sleep. This leads to reduced oxygen levels in the blood, further disrupting the sleep cycle and negatively affecting REM sleep. The lack of quality REM sleep can significantly impact dreaming, causing a reduction in dream intensity or altering the nature of dreams.
TBI can contribute to the development of sleep apnea by affecting the brainstem, which plays a role in regulating breathing. In addition to sleep apnea, other sleep disorders such as insomnia and restless leg syndrome may also develop after TBI, further affecting sleep quality and, by extension, the dreaming process.
NEUROCHEMICAL CHANGES AND THEIR EFFECT ON DREAMS
The brain’s neurotransmitter systems play a crucial role in regulating sleep and dreaming. TBI can result in alterations in the levels of neurotransmitters such as serotonin, dopamine and acetylcholine, which are all involved in the regulation of sleep and dream activity. Damage to these systems may lead to abnormal sleep cycles, less REM sleep and changes in the emotional tone of dreams.
Serotonin, for example, is critical for maintaining healthy sleep patterns and mood regulation. TBI-related disruptions in serotonin levels may contribute to sleep disturbances, nightmares and emotional instability in dreams. Similarly, changes in dopamine levels can affect motivation, reward systems and mood regulation, leading to more vivid or unusual dreams. Alterations in acetylcholine, a neurotransmitter essential for REM sleep, can directly impact the quality and frequency of dreaming.

NEUROPLASTICITY AND DREAMING POST-TBI
Neuroplasticity, the brain’s ability to reorganize itself and form new neural connections, plays a role in recovery after a traumatic brain injury. As the brain heals and compensates for areas of damage, it may restore some functions, including the ability to engage in normal sleep cycles and experience regular dreams. However, the extent of this recovery depends on the severity of the injury, the areas of the brain affected and the individual’s age and overall health.
In some cases, as neuroplasticity allows the brain to compensate for damage, individuals with TBI may experience a return of more vivid or coherent dreams. Conversely, some individuals may experience persistent disruptions in dreaming as the brain continues to adapt to the injury. The process of neuroplasticity is unique to each individual, and its impact on dreaming remains an area of ongoing research.
POTENTIAL TREATMENTS FOR DREAMING DISTURBANCES FOLLOWING TBI
While there is no definitive treatment to restore normal dreaming after a traumatic brain injury, several strategies may help manage the associated sleep disturbances and improve sleep quality, which, in turn, can support healthier dreaming.
Cognitive Behavioral Therapy for Insomnia (CBT-I): This type of therapy is often used to treat sleep disturbances in individuals with TBI. CBT-I helps individuals identify and address thoughts and behaviors that interfere with sleep, leading to improvements in overall sleep quality, which may also have a positive effect on dreaming.
Pharmacological Interventions: Medications such as antidepressants, antianxiety drugs or sleep aids may
be prescribed to individuals with TBI who suffer from nightmares or other sleep disturbances. These medications may help to regulate sleep patterns and reduce the frequency of nightmares.
Relaxation Techniques: Techniques such as meditation, deep breathing and progressive muscle relaxation may help individuals with TBI reduce stress and anxiety before sleep, leading to improved sleep quality and potentially less disturbing dreams.
Sleep Hygiene Education: Establishing a consistent sleep routine and creating a calm and comfortable sleep environment can improve sleep quality, leading to better recovery and less disruption to dreaming. Sleep hygiene strategies may include maintaining a consistent sleep-wake cycle, avoiding caffeine and alcohol before bedtime and minimizing screen time in the hours leading up to sleep.
Nightmare Management: Individuals who suffer from frequent nightmares related to TBI may benefit from therapies that focus on trauma resolution, such as EMDR (eye movement desensitization and reprocessing) or trauma-focused cognitive-behavioral therapy. These approaches aim to reduce the emotional impact of traumatic memories, potentially decreasing the frequency and intensity of nightmares.
IN CONCLUSION
The effects of traumatic brain injury on dreaming are varied and complex, reflecting the intricate nature of the brain’s sleep and memory systems. TBI can lead to disruptions in REM sleep, changes in dream content, increased nightmares and memory difficulties related to dream recall. These disturbances are influenced by various factors, including neurochemical changes, emotional responses to trauma and disruptions in brain regions responsible for sleep regulation.
Although many individuals with TBI experience significant changes to their dreams, there are effective strategies for managing these disturbances, including cognitive behavioral therapies, pharmacological interventions and lifestyle changes. By addressing the underlying sleep issues, it is possible to improve sleep quality, reduce nightmares and enhance the overall healing process following a traumatic brain injury. As research into the relationship between TBI and dreaming continues, a better understanding of these processes may lead to more targeted treatments and interventions.
Traumatic brain injury (TBI) is a serious and often life-threatening condition that results from a sudden blow or jolt to the head, causing damage to the brain. While many individuals who experience a TBI recover with appropriate treatment, in some cases, the injury can lead to death. The severity of the brain injury and the specific areas of the brain that are affected play a significant role in determining the outcome. Understanding how and why TBI can lead to death requires an exploration of the mechanisms of injury, the types of TBIs and the complications that can arise in the aftermath of a traumatic event.
MECHANISMS OF TRAUMATIC BRAIN INJURY
The brain is a delicate organ, and any significant trauma to the head can cause a range of injuries. TBI can occur through several mechanisms, including direct impact, acceleration-deceleration forces and rotational forces. A direct impact, such as a blow to the head from a fall or a car accident, can cause localized damage to the brain. The brain is cushioned by cerebrospinal fluid within the skull, but when an external force is strong enough, the brain can collide with the inside of the skull, causing bruising (contusion), swelling and even bleeding (hemorrhage).
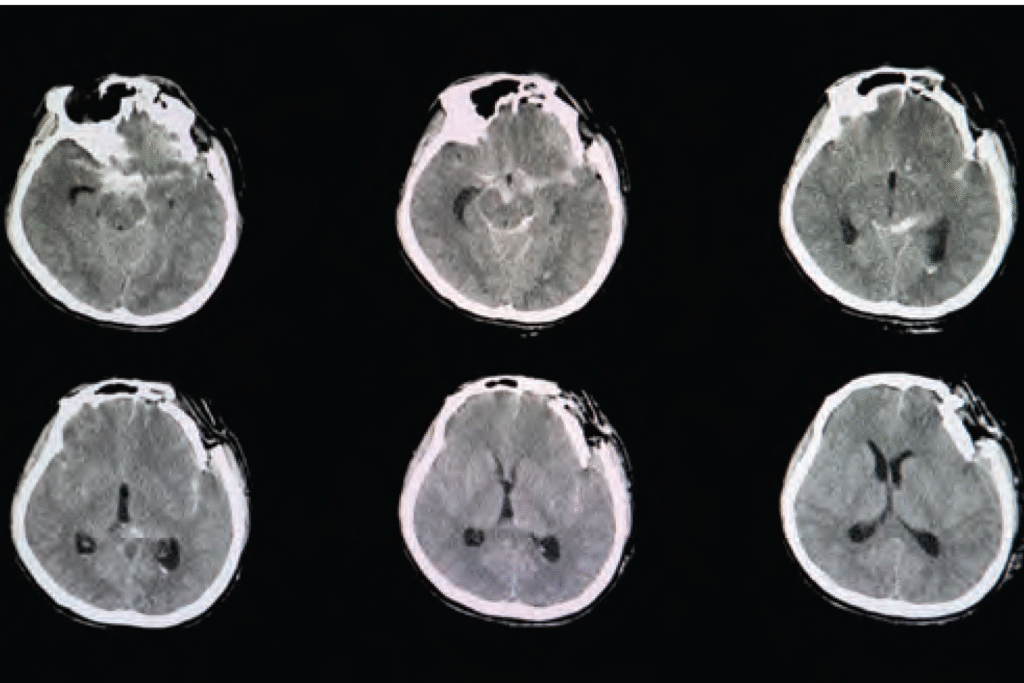
CT brain scan image of a patient with severe skull depression fracture at left frontal parietal area with left zygomatic arch and both maxillary sinuses fractures with small subarachnoidal hemorrhage.
Acceleration-deceleration injuries occur when the head is rapidly moved back and forth, as in a car crash or sports-related injury. This rapid motion causes the brain to shift within the skull, leading to damage to brain tissue, blood vessels and nerve fibers. Rotational forces, such as those caused by a sudden twisting motion, can tear nerve fibers (axons), resulting in diffuse axonal injury (DAI). DAI is one of the most severe forms of TBI and often results in long-term impairments or death. These mechanisms can cause damage to different regions of the brain, each of which plays a crucial role in basic life functions such as breathing, heart rate and consciousness.
TYPES OF TRAUMATIC BRAIN INJURY
TBI is classified into three main categories based on severity: mild, moderate and severe. Mild TBI, often referred to as a concussion, typically involves a brief loss of consciousness or confusion, with recovery expected within days to weeks. Moderate and severe TBIs, however, carry a much higher risk of complications and death. Moderate TBI can lead to lasting cognitive deficits and physical impairments, while severe TBI often involves significant brain swelling, bleeding and widespread tissue damage that can be fatal.
One of the most dangerous forms of TBI is a penetrating injury, in which an object, such as a bullet or sharp object, enters the skull and damages brain tissue. These injuries are often fatal because they cause immediate, severe damage to critical brain structures, leading to uncontrollable bleeding, infection and loss of function in vital areas of the brain. Subdural and epidural hematomas, which involve the accumulation of blood between the brain and the skull, are also life-threatening conditions that can result from moderate to severe TBI. These blood clots can put pressure on the brain, reducing blood flow and oxygen supply to vital brain regions, leading to brain death.
Brain Swelling and Increased Intracranial Pressure. One of the primary reasons that TBI can lead to death is brain swelling (cerebral edema), which can increase intracranial pressure (ICP). When the brain swells due to injury, there is limited space within the rigid skull to accommodate the expanding tissue. As a result, the pressure inside the skull rises, which can restrict blood flow to the brain and decrease the supply of oxygen and nutrients. This can lead to widespread brain cell death and irreversible brain damage.
COMPLICATIONS LEADING TO DEATH
In addition to brain swelling and increased ICP, there are several other complications that can arise from TBI and lead to death. These complications include hemorrhaging (bleeding) within the brain, infections and seizures. Intracranial bleeding, such as subdural or epidural hematomas, can quickly worsen and lead to irreversible brain damage. Hemorrhages can occur immediately after the injury or develop over time, making it crucial for medical professionals to monitor individuals with severe TBI closely.
Infections, particularly in cases of open head wounds or penetrating injuries, can also be fatal. Infections can spread rapidly within the brain, causing inflammation, tissue destruction and sepsis, which can lead to multi-organ failure and death. Seizures are another common complication of TBI, especially in individuals with moderate to severe injuries. Seizures can further damage brain tissue, increase ICP and contribute to other life-threatening conditions.
Traumatic brain injury can cause death through a combination of direct damage to the brain, swelling, bleeding and secondary complications such as infection and seizures. The severity of the injury, the areas of the brain affected and the individual’s overall health determine the likelihood of survival and recovery. Severe TBIs, particularly those involving significant brain swelling, hemorrhaging or penetration, carry the highest risk of death. Early intervention, medical management to control swelling and bleeding, and surgery to address complications can improve survival rates, but TBI remains a leading cause of death and long-term disability worldwide. Understanding the mechanisms of TBI and the risks involved highlights the importance of prevention, early detection and prompt medical treatment to reduce the potentially fatal consequences of head injuries.
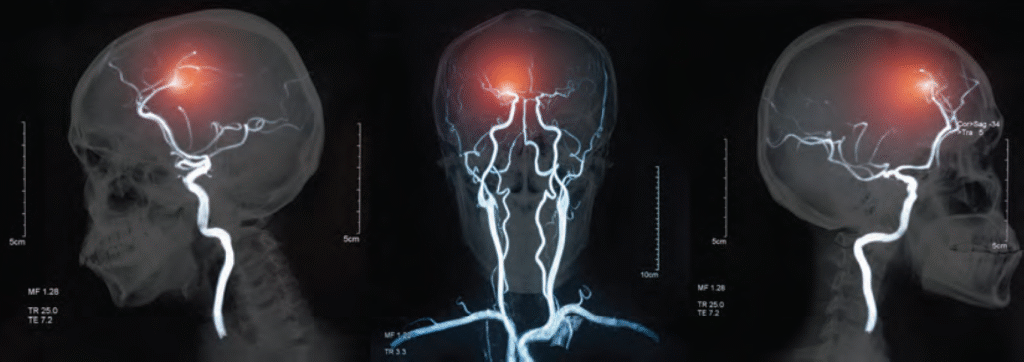
Awake craniotomy is an advanced surgical technique that is increasingly used to treat traumatic brain aneurysms, which are abnormal bulges or weakened areas in the walls of blood vessels within the brain and caused by traumatic injury. These aneurysms are particularly dangerous because they can rupture, leading to severe brain hemorrhage which may cause irreversible damage or even death. Traditionally, treating such aneurysms required traditional craniotomy, in which the skull is opened to access the brain, but awake craniotomy offers a more precise and safe alternative, especially when the aneurysm is located near critical brain structures.
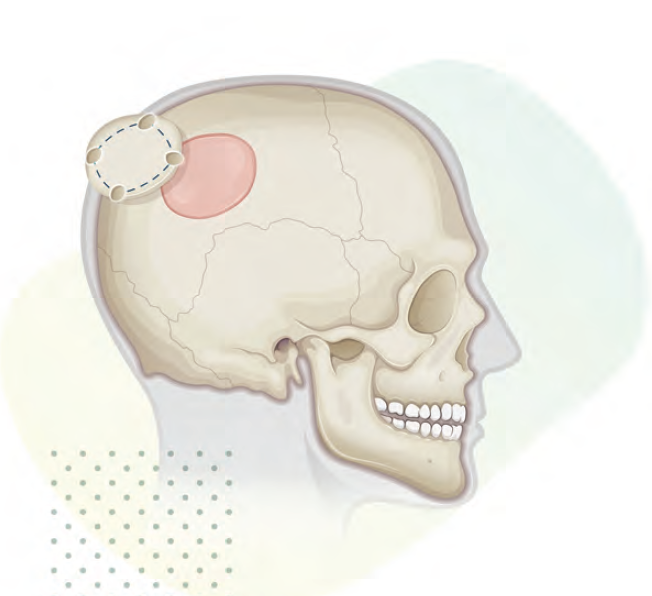
A craniotomy is a surgical operation in which a bone flap is temporarily removed from the skull to access the brain.
During an awake craniotomy, the patient is kept conscious throughout the procedure, but local anesthesia is administered to numb the scalp and skull. The patient is sedated enough to remain calm and comfortable, but remains alert and responsive for most of the surgery. This conscious state allows the surgeon to interact directly with the patient, performing neurological tests during the procedure. If the aneurysm is near regions of the brain responsible for essential functions such as speech, movement, or cognition, the surgeon can monitor the patient’s responses to stimulation, ensuring that vital brain areas are not damaged during the surgery.
For patients with traumatic aneurysms, awake craniotomy allows the surgical team to more effectively target the aneurysm while avoiding harm to crucial brain functions. For example, during surgery, the surgeon may ask the patient to speak or move a limb while stimulating specific brain areas to assess which parts of the brain control those functions. This real-time feedback enables the surgical team to navigate sensitive areas more carefully. The surgeon can make adjustments if they notice any adverse effects or if the patient shows signs of discomfort. This level of precision is particularly important for aneurysms located in complex or deep regions of the brain, where traditional surgery might risk significant damage to nearby structures.
One of the significant advantages of awake craniotomy is the ability to monitor the patient’s neurological status during surgery. In traditional surgeries, patients are typically under general anesthesia, making it impossible for the surgical team to assess the patient’s cognitive and motor functions in real time. In contrast, with awake craniotomy, the surgeon can adjust the procedure dynamically, reducing the risk
of complications such as paralysis, speech difficulties, or cognitive impairment. By ensuring that the brain is undamaged, the technique can result in better long-term outcomes and fewer complications after surgery. Patients are often able to recover more quickly and with less residual neurological damage, making this method particularly beneficial for those with traumatic brain injuries.
While awake craniotomy has many advantages, it also comes with challenges. The patient must be able to cooperate throughout the procedure, which may be difficult for some individuals, particularly those who experience anxiety or discomfort. Additionally, the procedure requires highly skilled surgical teams who can effectively communicate with the patient and monitor the brain’s response to stimulation. Despite these challenges, awake craniotomy remains a groundbreaking technique that significantly improves the treatment of traumatic aneurysms, offering a safer, more effective alternative to traditional surgical methods. By allowing surgeons to operate with increased precision and real-time feedback, awake craniotomy has become a key tool in treating brain aneurysms while minimizing the risk of long-term complications.
Stroke is a leading cause of disability and death worldwide. It occurs when there is a sudden interruption of blood flow to the brain, resulting in the death or damage of brain cells. While strokes have long been categorized as vascular events, they share similarities with traumatic brain injuries (TBIs) in their effects on brain tissue. Specifically, a stroke is now recognized as a type of non-traumatic brain injury (nTBI), a category that is not caused by direct physical trauma to the brain. This article explores the neuroscience behind stroke, its impact on the brain and why it is classified as an nTBI.
WHAT IS A STROKE?
A stroke occurs when there is a disruption in the blood supply to a part of the brain. This disruption can be due to two main mechanisms:
Ischemic Stroke: This type of stroke is caused by a blockage or narrowing of the blood vessels that supply the brain. A clot can form either in the brain itself (thrombotic stroke) or travel from another part of the body, such as the heart (embolic stroke).
Hemorrhagic Stroke: This occurs when a blood vessel in the brain bursts, leading to bleeding within the brain. The pooling of blood puts pressure on surrounding brain tissues, causing damage.
Both types of strokes share a common outcome: a lack of oxygen and nutrients to brain tissue, leading to cell death and neurological dysfunction. The primary difference between the two types is the mechanism causing the disruption in blood flow.
Ischemia and Oxygen Deprivation
When blood flow to a part of the brain is interrupted, the affected tissue becomes deprived of oxygen and glucose. These are essential for neurons to produce energy and function normally. Within minutes of ischemia, brain cells begin to suffer damage. The immediate effect is a phenomenon called cerebral ischemia, which causes a range of toxic processes within the brain.
THE NEUROSCIENCE OF STROKE: HOW IT AFFECTS THE BRAIN
To understand why stroke is considered an nTBI, it is important to examine the physiological mechanisms that occur during a stroke. Regardless of the type of stroke, the fundamental problem is the disruption of cerebral blood flow, which triggers a cascade of cellular and molecular events in the brain. Hemorrhagic Stroke: This occurs when a blood vessel in the brain bursts, leading to bleeding within the brain. The pooling of blood puts pressure on surrounding brain tissues, causing damage.
Both types of strokes share a common outcome: a lack of oxygen and nutrients to brain tissue, leading to cell death and neurological dysfunction. The primary difference between the two types is the mechanism causing the disruption in blood flow.
At the cellular level, neurons begin to experience energy failure, primarily due to a lack of adenosine triphosphate (ATP), which is crucial for maintaining normal cellular functions. Without ATP, the cell’s ion pumps malfunction, causing an imbalance of ions across the cell membrane. This leads to a phenomenon called excitotoxicity, where an excessive release of neurotransmitters, especially glutamate, results in an influx of calcium ions into the neuron. High calcium levels activate various enzymes that break down cellular structures, leading to cell death.
Stroke leads to inflammation in the affected brain region. This inflammation, called neuroinflammation, is triggered by the damage to brain cells and blood vessels. The activation of microglia, the brain’s resident immune cells, is a key component of this inflammatory response. Initially, microglia attempt to clear up dead cells and debris, but if the inflammation is prolonged, it can contribute to further brain injury by releasing pro-inflammatory cytokines and other toxic molecules.
Neuroinflammation is not only harmful in the acute phase of stroke but also contributes to long-term brain damage and recovery. The chronic inflammation that follows stroke has been implicated in the development of neurological deficits, cognitive decline and the progression of neurodegenerative diseases.
STROKE AS A NON-TRAUMATIC BRAIN INJURY (nTBI)
Traditionally, TBIs have been associated with external physical forces such as blows to the head, falls, or accidents. These external
forces result in direct trauma to the brain, leading to tissue damage and dysfunction. However, stroke, while not caused by a direct mechanical impact, can produce similar effects on brain tissue and functions. This has led to the recognition of stroke as a non-traumatic brain injury (nTBI).
An nTBI refers to any type of brain injury that is not the result of an external physical force but still leads to structural or functional damage to the brain. Strokes, whether ischemic or hemorrhagic, fit this definition because they result in significant brain injury due to the interruption of blood flow without any direct external impact on the brain.
WHY STROKE IS CONSIDERED AN NTBI
There are several reasons why stroke is categorized as an nTBI:
Similar Pathophysiology: Like traumatic brain injuries, stroke leads to neuronal cell death, neuroinflammation and long-term changes in brain structure and function. Both conditions cause damage to neurons and glial cells, leading to neurological deficits, cognitive impairments and emotional disturbances.
No External Trauma: Unlike TBIs, which are caused by external physical forces, strokes occur due to internal processes, such as blood clots or ruptured blood vessels. There is no direct impact on the skull or brain tissue from an external object, yet the effects on brain function can be just as devastating as a TBI.
Long-Term Consequences: Both stroke and TBI often result in long-term functional impairments, including motor deficits, sensory disturbances, cognitive decline and mood disorders. The recovery process for both conditions can be slow, requiring extensive rehabilitation and often leading to permanent disability.
Overlap in Risk Factors: Many of the risk factors for stroke overlap with those of TBI. For example, age, hypertension, diabetes and cardiovascular diseases are risk factors for both strokes and TBIs. Furthermore, individuals who have suffered a TBI are at an increased risk for stroke, further emphasizing the connection between the two conditions.
Impact on Brain Networks: Both stroke and TBI can disrupt the functioning of large-scale brain networks, affecting motor, sensory and cognitive functions. These disruptions can lead to widespread changes in brain connectivity, which is often associated with neurological deficits and difficulties in recovery.
CLINICAL IMPLICATIONS AND TREATMENT OF STROKE AS AN NTBI
Recognizing stroke as an nTBI has important clinical implications. It highlights the need for timely intervention to prevent further brain damage and improve outcomes. For example, the use of thrombolytic therapy (clot-busting drugs) and mechanical thrombectomy in ischemic stroke can restore blood flow and limit the extent of brain damage, much like how early intervention in TBI can prevent secondary injury.
Additionally, the rehabilitation of stroke patients often involves similar strategies used for TBI patients, including physical therapy, occupational therapy and neuropsychological interventions. The goal is to help patients recover lost functions and adapt to any remaining disabilities.
IN CONCLUSION
Stroke is a complex neurological event that results in the disruption of blood flow to the brain, leading to cell death, inflammation, and long-term neurological impairment. While strokes are caused by vascular issues and not external trauma, they share many similarities with traumatic brain injuries in terms of
their pathophysiology, clinical outcomes and impact on brain function. For these reasons, stroke is increasingly recognized as a form of non-traumatic brain injury (nTBI), and understanding its mechanisms can help improve treatment and rehabilitation strategies for those affected. By viewing stroke through the lens of nTBI, we can better address the needs of patients, leading to improved care and recovery outcomes.
Scuba diving is an exciting and thrilling activity that allows individuals to explore the wonders of the underwater world. However, beneath its allure, scuba diving may pose certain risks to the brain, especially when improper techniques, rapid ascension, or inadequate decompression protocols are involved. While acute decompression sickness (DCS) is commonly discussed as a significant threat, brain damage from scuba diving can occur even in the absence of acute symptoms. This article explores the potential brain damage caused by scuba diving, both with and without the presence of acute decompression sickness, and provides precautions to minimize these risks.
BRAIN DAMAGE IN THE PRESENCE OF ACUTE DECOMPRESSION SICKNESS
Acute decompression sickness, often referred to as “the bends,” is a condition that occurs when nitrogen, which is absorbed into the body during a dive, forms bubbles in the bloodstream upon rapid ascent. These bubbles can obstruct blood vessels and lead to a range of neurological symptoms, including brain damage. When a diver ascends too quickly, the rapid reduction in pressure causes nitrogen to come out of solution and form bubbles that can accumulate in the brain, spinal cord and other tissues.
The brain is particularly vulnerable to these gas bubbles because they can disrupt the normal flow of blood, depriving neural tissue of oxygen and leading to ischemic injury. The severity of brain damage from DCS depends on several factors, including the depth of the dive, the duration of the dive and the speed of ascent. Prolonged exposure to high-pressure environments can increase the likelihood of forming gas bubbles that are large enough to cause tissue damage.
Symptoms of DCS affecting the brain include dizziness, confusion, loss of coordination, visual disturbances, seizures and, in extreme cases, loss of consciousness. If left untreated, these symptoms can lead to permanent brain damage or even death. The damage occurs because the bubbles obstruct the small blood vessels in the brain, preventing proper blood flow and oxygen delivery to the neural tissue. This lack of oxygen (hypoxia) can cause neurons to die, leading to cognitive impairments, motor deficits and other long-term neurological issues.

BRAIN DAMAGE IN THE ABSENCE OF ACUTE DECOMPRESSION SICKNESS
Even when acute decompression sickness is not present, there are still risks of brain damage associated with scuba diving. One potential mechanism for this type of brain injury is chronic exposure to high-pressure environments, which can lead to oxygen toxicity, a condition that results from breathing high concentrations of oxygen at elevated pressures. This condition can damage brain cells by producing reactive oxygen species (ROS), which are highly reactive molecules that can cause cellular damage, inflammation and cell death.
Another potential risk factor for brain damage in the absence
of DCS is repetitive exposure to diving environments without adequate recovery periods. This can lead to a condition known as “chronic dive syndrome,” which may involve subtle but cumulative neurological changes. Some studies suggest that frequent diving without sufficient time for the body to off-gas nitrogen can result in low-level nitrogen buildup in the brain, which could potentially impair cognitive function over time.
Additionally, the physiological stress associated with diving, such as the increased workload on the heart and the body’s need to adapt to fluctuations in pressure, may exacerbate pre-existing brain conditions or contribute to vascular changes that compromise brain health. These factors, when combined with dehydration, fatigue, or hypothermia from cold water exposure, can lead
to minor brain injuries that accumulate over time, potentially resulting in long-term cognitive dysfunction.
POTENTIAL BRAIN DAMAGE FROM NITROGEN NARCOSIS
Another critical consideration in relation to brain health while scuba diving is nitrogen narcosis. This condition, commonly referred to as the “rapture of the deep,” occurs when nitrogen becomes more soluble at high pressures, affecting the central nervous system and leading to symptoms similar to alcohol intoxication. At depths greater than 30 meters (100 feet), divers may experience impaired judgment, motor coordination and cognitive function. In severe cases, nitrogen narcosis can cause confusion, hallucinations and loss of consciousness, increasing the risk of accidents and brain injury.
While the effects of nitrogen narcosis are typically reversible upon ascent, repeated exposure to the condition may contribute to long-term neurological changes. Some researchers suggest that chronic nitrogen narcosis could lead to subtle cognitive deficits or an increased risk of developing neurodegenerative disorders in the long term, though further research is needed to fully understand these risks.
PRECAUTIONS TO PREVENT BRAIN DAMAGE FROM SCUBA DIVING
While the potential for brain damage during scuba diving is a serious concern, there are several precautions divers can take to minimize the risks and ensure safe diving practices. These include proper training, adhering to safe diving limits, and taking steps to manage nitrogen exposure.
Proper Training and Certification: Ensuring that all divers are properly trained and certified through reputable organizations, such as PADI (Professional Association of Diving Instructors) or NAUI (National Association of Underwater Instructors), is essential. Certified divers are taught safe diving practices, including the importance of controlling ascent rates and adhering to depth limits.
Slow and Controlled Ascent: One of the most crucial precautions to avoid decompression sickness and potential brain injury is to ascend slowly. Divers should always follow the recommended ascent rates (no faster than 9 meters per minute or 30 feet per minute) and make safety stops at 3 to 5 meters (10 to 15 feet) to allow nitrogen to safely leave the body.
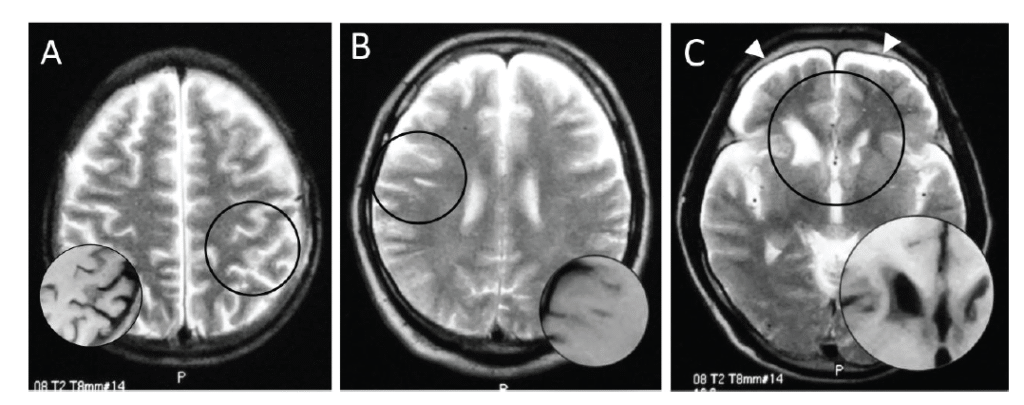
Magnetic resonance images of brains of three Ama divers: hyperintense area on T2-weighted image (circle), corresponding to hypointensity on T1-weighted image (inset). A patchy shadow in the left parietal cortex (A, No. 2), a linear subcortical lesion in the right frontal lobe (B, No. 5), and deformity of bilateral caudate heads and subdural fluid collection (allow heads) (C, No. 11).
Decompression Stops and Tables: Using dive tables or dive computers is critical to ensure that divers do not exceed safe no-decompression limits. These tools help track the nitrogen load accumulated during the dive, providing guidance on when and where to make decompression stops to prevent DCS.
Adequate Rest Between Dives: Giving the body enough time to off-gas nitrogen before the next dive is vital. Avoiding multiple dives on a single day or diving on consecutive days without adequate surface intervals can reduce the risk of nitrogen buildup and the potential for neurological damage.
Oxygen Exposure Management: Limiting exposure to oxygen-rich environments, especially during deep dives, is essential to prevent oxygen toxicity. Divers should avoid prolonged stays at depths greater than 40 meters (130 feet) and be cautious when diving with enriched air (“nitrox”), ensuring that oxygen partial pressures do not exceed safe levels.
Hydration and Avoiding Fatigue: Staying well-hydrated and ensuring adequate rest before and after dives is important for maintaining cognitive function and reducing stress on the body. Dehydration and fatigue can increase susceptibility to diving-related injuries, including those affecting the brain.
Post-Dive Monitoring: After a dive, monitoring for symptoms of DCS, such as dizziness, confusion or difficulty breathing, is essential. If any symptoms occur, immediate medical attention should be sought to prevent potential brain damage or other serious complications.
IN CONCLUSION
Scuba diving can offer a rich and rewarding experience, but it is not without its risks. The potential for brain damage exists both with and without the presence of acute decompression sickness, making it essential for divers to take proper precautions to minimize harm. By following established safety protocols, receiving proper training, managing exposure to nitrogen and oxygen and ensuring adequate rest, divers can significantly reduce the risks associated with diving and protect their brain health. With the right approach, scuba diving can remain a safe and enjoyable activity for both recreational and professional divers alike.
Mild traumatic brain injury (mTBI), often referred to as a concussion, is one of the most common and underdiagnosed injuries in both sports and everyday life. Traditionally, concussions have been diagnosed based on clinical symptoms and patient history, which may often be subjective and prone to misinterpretation. This uncertainty has prompted extensive research to find more objective and accurate diagnostic tools for mTBI, with molecular markers emerging as a promising solution. The identification of these biomarkers could potentially revolutionize the way concussions are diagnosed, offering a path toward definitive, objective diagnosis. This article explores the current state of research on molecular markers for mTBI and their role in making concussion diagnosis a reality.
THE CHALLENGE OF DIAGNOSING MTBI
A concussion results from a blow to the head or a jolt to the body that causes the brain to move rapidly inside the skull, leading to temporary disruption in brain function. The symptoms of a concussion are wide-ranging, including headaches, dizziness, confusion, nausea and cognitive difficulties such as memory problems and difficulty concentrating. Importantly, many symptoms are not visible, and they can evolve over hours or days, making it challenging to assess the extent of the injury in real time.
Currently, the diagnosis of mTBI relies heavily on clinical evaluations, such as the Glasgow Coma Scale (GCS), symptom checklists, and imaging tests like CT or MRI scans. However, these methods have limitations. GCS scores are useful in assessing the severity of brain injury, but they do not differentiate between mild and moderate brain injuries effectively. Imaging techniques, while excellent at detecting more severe brain injuries, often fail to show any abnormalities in the case of mTBI, as the damage caused by concussions is typically microscopic.
This lack of diagnostic precision can lead to underdiagnosis, where individuals with concussions continue to engage in physical activity, risking further injury, or overdiagnosis, where individuals are sidelined unnecessarily. Both scenarios highlight the need for a more objective method to diagnose concussions accurately.
THE PROMISE OF MOLECULAR MARKERS
In recent years, research into the molecular mechanisms underlying mTBI has revealed that certain proteins and molecules are released into the bloodstream or cerebrospinal fluid (CSF) shortly after a brain injury. These biomarkers, or molecular markers, can provide crucial information about the extent and nature of brain injury. Unlike traditional methods, molecular markers offer a window into the biological changes occurring at the cellular level following a concussion.

The use of molecular markers as a diagnostic tool for mTBI holds immense promise because it can provide a more definitive and objective measure of injury. Unlike symptom-based assessments, which may be influenced by the patient’s ability to report symptoms and the subjective interpretation of healthcare providers, molecular markers are tangible and measurable indicators of physiological changes. Additionally, the detection of molecular markers can help monitor recovery, guide clinical decisions and aid in preventing second-impact syndrome, a potentially fatal condition that occurs when an individual sustains a second concussion before the first one has healed.
KEY MOLECULAR MARKERS FOR MTBI
Numerous molecular markers have been identified in the search for reliable diagnostic tools for mTBI. These markers typically fall into categories based on the nature of the substances they represent, such as neuronal proteins, glial markers, or molecules associated with inflammation. Below are some of the most promising molecular markers:
- Glial Fibrillary Acidic Protein (GFAP)
GFAP is a protein found in the glial cells of the brain, which provide support and nourishment to neurons. When the brain is injured, GFAP is released into the bloodstream as glial cells are damaged. Elevated levels of GFAP have been shown to correlate with the severity of brain injury. In fact, research has shown that GFAP levels can be measured in the blood within hours
of a concussion and provide valuable insights into the injury’s severity. GFAP, along with other markers, may become a key biomarker for mTBI diagnosis. - S100B Protein
S100B is a calcium-binding protein that is primarily expressed in glial cells and neurons. When the brain is injured, S100B is released into the bloodstream, making it a potential marker for detecting mTBI. Elevated levels of S100B in the blood have been associated with both mild and severe brain injuries. This biomarker has been widely studied, and although its specificity for mTBI remains a topic of ongoing research, its use in conjunction with other markers could significantly improve diagnostic accuracy. - Ubiquitin C-terminal Hydrolase L1 (UCH-L1)
UCH-L1 is an enzyme found in neurons that plays a role in protein degradation. In the event of neuronal injury, UCH-L1 is released into the bloodstream. Several studies have demonstrated that increased levels of UCH-L1 in blood samples are strongly associated with brain injury, and elevated concentrations have been observed following both acute and subacute phases of mTBI. UCH-L1 is particularly promising because it can be detected shortly after the injury and may provide an early indicator of concussion severity. - Tau Protein
Tau is a protein that stabilizes microtubules in neurons. Following a brain injury, tau can become hyperphosphorylated, leading to its detachment from microtubules and subsequent release into the bloodstream. Elevated tau levels are typically associated with more severe forms of brain injury and are considered a hallmark of neurodegenerative diseases such as Alzheimer’s. However, its role in mTBI has garnered significant attention. Elevated tau levels can serve as a potential marker for detecting concussion-related brain injury, particularly when combined with other biomarkers.
- Neurofilament Light Chain (NfL)
NfL is a structural protein found in neurons, and its release into the bloodstream has been linked to axonal injury. As axons are damaged following mTBI, NfL levels in the blood rise. Several studies have demonstrated that NfL concentrations are elevated in patients with mTBI and can provide valuable information about the extent of axonal injury. NfL may offer a broad and reliable method for detecting brain injuries, especially mild ones, that would not otherwise be visible using conventional imaging techniques.
CLINICAL IMPLICATIONS OF MOLECULAR MARKERS FOR MTBI DIAGNOSIS
The ability to identify and measure these molecular markers in blood or CSF opens up several exciting possibilities for improving concussion diagnosis and management. One of the most significant advantages of molecular markers is their ability to detect mTBI early, even in the absence of visible symptoms or abnormalities on standard imaging. This early detection could allow healthcare professionals to make timely decisions about whether an athlete or patient should rest, undergo further testing, or return to activity.
Furthermore, molecular markers can be used to track recovery. By measuring biomarker levels over time, clinicians can assess whether the brain is healing appropriately or if additional treatment or rest is needed. This monitoring could help prevent the long-term consequences of multiple concussions, including chronic traumatic encephalopathy (CTE) and other neurodegenerative diseases.
Molecular markers may also reduce the reliance on subjective symptom reporting, which may be inconsistent, particularly among athletes who may be reluctant to report their symptoms due to the desire to continue playing. By providing an objective, biological measure of injury, molecular markers could help ensure that individuals who sustain a concussion are appropriately managed and protected from further harm.
IN CONCLUSION
The identification of molecular markers for mTBI is poised to transform concussion diagnosis from a largely subjective process into one that is objective and precise. By providing a more accurate and timely assessment of brain injury, molecular markers have the potential to improve patient care, reduce the risk of further injury, and enhance recovery outcomes. While more research is needed to refine these biomarkers and establish standardized testing protocols, the progress made so far brings us closer to the day when definitive concussion diagnosis is a reality. With continued advancements in molecular biology, it may soon be possible to accurately diagnose and manage mTBI with the same level of certainty that we apply to other medical conditions.
Traumatic brain injury (tbi) can have significant and long-lasting effects on communication. Cognitive impairments resulting from TBI can impact an individual’s ability to express thoughts clearly, understand language and engage in social interactions. However, recent advancements in digital communication and technology have opened new pathways to assist individuals with TBI. One of the most promising tools for improving communication in this population is the use of emojis. These small, expressive symbols can help bridge communication gaps, offering a simple, effective means for individuals with TBI to express emotions, convey meaning and engage with others.
UNDERSTANDING TRAUMATIC BRAIN INJURY AND ITS IMPACT ON COMMUNICATION
TBI occurs when a sudden trauma causes damage to the brain, which can result from a fall, accident, sports injury, or violent impact. The effects of TBI vary widely depending on the severity of the injury and the area of the brain affected. Common symptoms include memory loss, difficulty concentrating, emotional instability and problems with speech and language.
For many individuals with TBI, language processing and expression become major challenges. These individuals may struggle to find the right words, organize their thoughts, or engage in fluid conversation. In severe cases, individuals may be unable to communicate at all, relying on nonverbal forms of expression. The resulting isolation and frustration may have a profound impact on the emotional well-being of individuals with TBI, further exacerbating communication difficulties.
THE ROLE OF EMOJIS IN COMMUNICATION
Emojis are small, digital images or icons used to convey emotions, ideas, or reactions in electronic communication. Emojis have become an integral part of texting, social media interactions and online conversations. Their simplicity and visual appeal make them particularly effective for conveying emotions quickly and clearly, making them an ideal tool for individuals with communication challenges.
Emojis help bridge the gap between text-based communication and nonverbal cues which are often lost
in written communication. For individuals with TBI,
using emojis can provide an intuitive, accessible way to communicate their feelings, reactions and thoughts, even when words may fail them. They can add a layer of emotional context to text messages, helping others understand the underlying sentiment behind the words.
HOW EMOJIS BENEFIT INDIVIDUALS WITH TBI
Nonverbal Communication Enhancement: One of the key struggles individuals with TBI face is the difficulty in expressing emotions or conveying the intended tone. In speech and written communication, individuals with TBI may find it challenging to express sadness, joy, anger, or excitement in a way that is easily understood by others. Emojis serve as a visual representation of these emotions, providing a clear and direct way for individuals to express themselves. For example, a simple smiley face can indicate happiness or contentment, while a sad face can convey sadness or frustration. This nonverbal support allows individuals to communicate more effectively, even when their verbal skills are impaired.
Improved Clarity in Communication: TBI can often cause cognitive difficulties, including problems with word-finding, memory and sentence construction. In these instances, emojis may help fill in the gaps, allowing individuals to convey meaning without needing to rely solely on words. For example, if someone struggles to describe an event, they may choose to pair a thumbs-up emoji with a few words, indicating approval or agreement. This visual support enhances the clarity of the message, helping to reduce misunderstandings and ensure effective communication.
participate in conversations. The use of emojis can encourage social interaction by lowering the barriers to communication. Emojis provide a less intimidating way for individuals with TBI to engage in digital conversations. A single emoji can be an easy and approachable way to respond to others, express gratitude, or show interest in a topic, even when verbal communication feels overwhelming or difficult.
Reducing Emotional Frustration: Difficulty communicating effectively can lead to frustration, anxiety and depression for individuals with TBI. The inability to express one’s thoughts and emotions in a clear manner may create feelings of helplessness. Emojis offer a way to quickly express how one feels without the pressure of finding the right words. By using emojis, individuals can feel more in control of their communication, which can reduce feelings of frustration and help them maintain emotional stability.
Supporting Cognitive Rehabilitation: Cognitive rehabilitation is an important part of the recovery process for individuals with TBI. Therapy often focuses on improving cognitive functions such as memory, attention and problem-solving skills. Emojis can play a role in this process by providing
a visual tool to reinforce cognitive exercises. For example, therapists may encourage patients to use specific emojis as part of their rehabilitation program, helping them remember and recall emotions, identify appropriate responses and practice communication in a safe, controlled environment.
Enhancing Digital Literacy: In today’s world, digital communication is an essential part of daily life. For individuals recovering from TBI, gaining comfort and confidence with digital platforms is often an important goal. Learning how to use emojis as part of text-based communication can enhance digital literacy, making it easier for individuals to engage with others on social media, send messages to loved ones and participate in online communities. Emojis serve as a nonverbal tool that complements traditional digital communication, helping individuals feel more confident and capable in their online interactions.
CASE STUDIES AND REAL-WORLD APPLICATIONS
A growing body of research and anecdotal evidence suggests that emojis have a positive impact on communication for individuals with TBI. For example, a study conducted with individuals recovering from TBI found that the use of emojis improved the clarity and emotional tone of their written messages. Participants reported feeling more confident in their ability to express emotions and connect with others. Additionally, caregivers and family members noted that emojis helped reduce the frustration associated with communication difficulties, leading to improved relationships and better emotional well-being.
In another case, therapists working with individuals who had sustained TBIs in accidents or sports injuries integrated emojis into their rehabilitation programs. By using emojis to represent different emotions or actions, individuals were able to engage more effectively with cognitive exercises. The therapists noted that this simple tool helped reinforce lessons about emotional expression, improved social skills and encouraged more interactive communication.
Moreover, families of individuals with TBI have reported that the use of emojis has helped maintain relationships by providing an easier way for loved ones to communicate. Emojis have become an essential tool for those supporting persons with TBI, offering a nonverbal way to check in, offer support, or show empathy without overwhelming the individuals with excessive verbal demands.
IN CONCLUSION
Emojis represent a simple yet powerful tool for individuals with traumatic brain injury to enhance communication, express emotions and reduce social isolation. By offering a visual and intuitive means of communication, emojis help individuals with TBI overcome language barriers, alleviate frustration and engage more effectively with others. As digital communication continues to play an increasingly important role in modern society, the use of emojis can be an essential part of the recovery and rehabilitation process for individuals with TBI. While they may not be a cure-all, emojis provide a meaningful way to support communication and improve quality of life for those affected by TBI, offering a small yet significant step toward a more inclusive and understanding world.
Traumatic brain injury (TBI) is a common and often serious condition that occurs in accidents involving an impact to the head. In many cases, the victim does not realize the full extent of their injury until months or even years after the trauma has occurred and symptoms surface. This can result in great personal suffering and even monetary repercussions for example a personal injury case being settled before it is clear that the victim has a brain injury.
Although fragile bones can mend, TBI can leave a person’s life irrevocably changed, permanently damaging their relationships, work, mental capacity, and quality of life. For these reasons, it is important for those who have experienced head trauma to be acutely aware of the potential of TBI so that they may seek out treatment as soon as possible. TBIs can range from mild (concussions) to severe, with causes ranging from simple slip and fall injuries or major motor vehicle collisions to full-contact sports injuries.
From a physiological perspective, TBI trauma occurs as a consequence of a sudden acceleration or deceleration or by a complex combination of both movement and sudden impact. Depending on the severity of the injury, the required treatment may be minimal or multidimensional and can include various types of intervention. This is called team-based treatment and is defined as professionals from a range of disciplines working together to deliver comprehensive care that addresses as many of the patient’s needs as possible. In this treatment model, care can be provided by a range of professionals functioning as a team under one organizational umbrella or by professionals from a range of organizations brought together as a unique team. As a patient’s condition changes over time, the composition of the team may change to reflect the changing clinical and psychosocial needs of the patient.
There are many options available to doctors when taking a multifaceted approach to diagnosing and treating TBI. Symptom triggers can be successfully identified through cognitive therapy, surgical intervention is also appropriate in some cases, and medication can play an important role in managing symptoms.
We talked to two authorities in their fields, Dr. Fardad Mobin, M.D. (a neurosurgeon), and Dr. Rod Amiri, M.D. (a neuropsychiatrist) to learn how these two specialties contribute to the successful treatment of TBI.
In more severe cases of TBI, neurosurgery may be a necessary part of treatment. A neurosurgeon is a medical doctor who specializes in evaluating, diagnosing, and treating conditions of the brain, spine, and nervous system. Neurosurgeons have extensive training, knowledge, and experience performing some of the most complex surgical procedures the human body can undergo and can also diagnose and treat conditions affecting the structures that support the nervous system including the skull, spinal vertebrae, spinal discs, and blood vessels.
Dr. Fardad Mobin, M.D. is a highly-skilled, board-certified neurosurgeon. He has performed over 2,000 surgeries and is recognized for his exceptional operative skills as well as his excellent patient care. Dr. Mobin is a graduate of the Rensselaer Polytechnic Institute in Troy, New York, holds a medical degree from the University of California Davis School of Medicine, and has completed a fellowship at the University of California, Los Angeles.
TBI TIMES: How would you describe a neurosurgical approach to the treatment of TBI?
DR. Mobin: Neurosurgeons are at the frontline when it comes to caring for TBI patients. We are routinely consulted by emergency room physicians and trauma surgeons to take an active role in the management of individuals with acute traumatic brain injury, from mild uncomplicated head injuries to severe life-threatening intracranial injuries. The first goal of neurosurgical intervention is to relieve the build-up of pressure within the enclosed cranium and prevent brain herniation. The next course of action is to rescue the brain tissue at risk of irreversible damage. Neurosurgical intervention consistently involves control of intracranial pressure by performing craniotomies to control and evacuate intracranial bleeds and restore normal pressure within the cranium. The neurosurgeon is an active player in post-operative critical care, working hand in hand with the ICU team to manage the multitude of parameters that are critical to the recovery of TBI patients.
TBIT: Specifically, how do neurosurgeons neuropsychiatrists work together to treat TBI?
DM: Individuals with TBI can suffer from an array of brain functionality issues, often manifesting as personality change, short-term or long-term memory loss, cognitive decline, and difficulty with focus and information processing. Neuropsychiatrists can perform detailed cognitive testing to link the observed deficits to any underlying structural injuries. This information will then help guide the patient’s rehabilitation program.
TBIT: Can neurosurgery alone ever successfully treat TBI? DM: No. Both acute and chronic phases of TBI require a multidisciplinary treatment team. Neurosurgeons play a very important role in the treatment of both the acute and chronic phases of TBI, however, the coordinated care of several disciplines including neurosurgeons, trauma surgeons, physiatrists, physical therapists, neuroradiologists, neurocognitive psychiatrists, and speech therapists, to name a few, are necessary for the successful treatment of TBI.
TM: Is neurosurgery used in the treatment of mild, moderate, and severe TBI?
DM: Yes. The discipline of neurosurgery places a great deal of concentration on the treatment of acute brain injury, and neurosurgical training concentrates on both surgical and medical care of TBI. Neurosurgeons are uniquely positioned to conduct life-saving procedures to relieve intracranial pressure and employ the critical care necessary to prevent secondary brain damage. For more information on Dr. Mobin: (310) 829-5888 or spinesurgeonla.com.
Neuropsychiatrists also play an essential role when treating patients who have experienced TBI and are trained in the diagnosis and treatment of a wide range of conditions. The main focus of neuropsychiatry
is understanding the psychological and psychiatric symptoms that arise from brain injury and disease and how to go about treating them.
Dr. Rod Amiri, M.D. is a board-certified psychiatrist and diplomate of the American Board of Psychiatry and Neurology as well as the American Board of Addiction Medicine. Based in Los Angeles, California, Dr. Amiri Is also an injury specialist (CBIS) certified by the Brain Injury Association of America. Committed to the ever-evolving and growing understanding of the psychological and psychiatric impacts of TBI, his concentration on the psychological symptoms of brain injury and disease gives him a unique perspective when it comes to treating the mental health side effects of TBI.
TBI TIMES: In your opinion, how important is a multidisciplinary approach to
the treatment of TBI?
DR. AMIRI: When we take a multifaceted approach to treating the symptoms of TBI we have many tools at our disposal, increasing the odds of a patient making a successful recovery. Cognitive therapy is important to identify symptom triggers, in many cases, surgical intervention is warranted, and at times medication plays a role in managing symptoms. This is why it is so important to approach treatment from many angles.
TBIT: What is the connection between the specific nature of a TBI and the psychological symptoms a patient may experience?
DA: There is no question that physical damage to the brain can cause cognitive, emotional, and behavioral issues. Research has shown that the specific area of the brain affected by TBI translates directly to the potential side effects a patient may experience. For example, injuries on the right side of the head are more likely to cause manic symptoms, injuries to the left side of the head are more likely to cause depressive symptoms, and frontal-cortex injuries can lead to personality-disrupting symptoms such as impulsivity and disinhibition.
TBIT: If patients experience psychological symptoms associated with TBI, what might they expect?
DA: The short- and long-term psychological effects depend on the severity and location of the injury as well as the age of the patient and their overall mental state before the TBI, especially if there were pre-existing psychological or functionality issues. The ideal treatment approach depends on multiple factors. This is why a team approach is advantageous so that we can cover as many bases as possible to benefit the patient.
TBIT: What role does psychiatric medication play in
TBI recovery?
DA: Medication is just one component of TBI treatment. A simple analogy would be that therapy is akin to an elite athlete’s training while finding the ideal medication for a patient is akin to finding the ideal diet for that athlete. Take Michael Phelps, for instance. He would not have been successful at the Olympics if he was eating unhealthy foods. He needed a certain diet to achieve success.
Although the medications we use in TBI patients are often the same as those used to address primary psychological disorders, it is important to start a TBI patient on a very low dosage. This is because TBI-induced psychological symptoms are inherently different from typical psychiatric issues. For more information on Dr. Amiri: (424) 360-0155 or connectwellnesscenter.com.
Contribute to the TBI Times